Advertisement
Grab your lab coat. Let's get started
Welcome!
Welcome!
Create an account below to get 6 C&EN articles per month, receive newsletters and more - all free.
It seems this is your first time logging in online. Please enter the following information to continue.
As an ACS member you automatically get access to this site. All we need is few more details to create your reading experience.
Not you? Sign in with a different account.
Not you? Sign in with a different account.
ERROR 1
ERROR 1
ERROR 2
ERROR 2
ERROR 2
ERROR 2
ERROR 2
Password and Confirm password must match.
If you have an ACS member number, please enter it here so we can link this account to your membership. (optional)
ERROR 2
ACS values your privacy. By submitting your information, you are gaining access to C&EN and subscribing to our weekly newsletter. We use the information you provide to make your reading experience better, and we will never sell your data to third party members.
Personalized Medicine
Diagnostics-Drugs Pairings Advance Personalized Medicine
Companion diagnostics matching patients with drugs are becoming mainstream
by Celia Henry Arnaud
July 23, 2012
| A version of this story appeared in
Volume 90, Issue 30

Within two weeks last August, the U.S. Food & Drug Administration approved two new cancer drugs: Roche’s Zelboraf, also called vemurafenib, for metastatic melanoma and Pfizer’s Xalkori, or crizotinib, for non-small-cell lung cancer. What sets those drugs apart from other cancer treatments is the requirement that physicians use a diagnostic test to determine whether each one is right for a patient. In the year since their approval, the two drugs have become poster children for personalized medicine and for what the industry calls “companion diagnostics.”
FDA defines companion diagnostics as analytical tests that are required for the safe and effective use of a drug. These assays measure a biomarker such as DNA or a protein to stratify the patient population and identify those individuals most likely to benefit or experience side effects from a drug. On the basis of test results, patients can be included in or excluded from clinical trials and prescriptions. Such tests become necessary when there’s no other way to identify appropriate patients.
Xalkori and Zelboraf are not the first drugs to use companion diagnostics. That honor goes to Herceptin, Genentech’s drug for HER2 (human epidermal growth factor receptor 2)-positive breast cancer, which was approved in 1998. What was once unusual is now poised to become mainstream. On July 6, FDA approved a companion diagnostic from Qiagen to identify appropriate patients for a new indication for the cancer drug cetuximab, which is comarketed by Eli Lilly & Co. and Bristol-Myers Squibb as Erbitux.
Last summer, FDA released a draft guidance document on companion diagnostics for industry and FDA staff to clarify when such tests will be required for regulatory approval and to outline the regulatory process. But “we’re not pushing anybody in this direction,” says Elizabeth A. Mansfield, director of personalized medicine in the Office of In Vitro Diagnostic Device Evaluation & Safety in FDA’s Center for Devices & Radiological Health. However, some companies are designing clinical trials this way, she points out, because “they want to be able to select a population that’s going to respond in a robust enough way to convince everyone that their drug actually works.”
Pharmaceutical companies are embracing codevelopment of drugs and diagnostics because that’s where the science is leading them. “We’ve been treating all tumors alike,” says Richard E. Buller, vice president for translational oncology at Pfizer, “but we have data that says they’re not all alike.”
For example, a receptor might be expressed in one type of breast cancer but not in another. On the basis of the receptor’s expression, breast cancer can be divided into multiple subtypes, including HER2 positive or estrogen receptor positive, among others. By correctly identifying patients, pharma companies can target these different subtypes with different drugs.
“We’re following the scientific understanding of disease into the clinic,” says Garret M. Hampton, Genentech’s senior director of oncology biomarker development.
Kitted out
Diagnostic labs use reagent kits from Abbott and Roche to test whether cancer patients have mutations that make Xalkori and Zelboraf, respectively, effective for them.



Cancer is the family of diseases for which that scientific understanding is most advanced. The experience of Roche and Pfizer in developing Zelboraf and Xalkori, respectively, underscores how companies are using the knowledge to develop drugs for forms of cancer that have had limited treatment options.
Roche’s path began in 2002, when scientists discovered that mutations in the BRAF gene, which encodes an enzyme involved in cell signaling, are involved in some cases of metastatic melanoma. By 2005, Plexxikon, Roche’s partner in developing Zelboraf, had designed a drug to inhibit the mutated B-Raf kinase expressed by the aberrant gene. Plexxikon contacted Roche Molecular Systems to see whether the diagnostics company could develop a test for the mutation. “We started to work on it right away,” says Walter H. Koch, head of research at Roche Molecular Systems. Within a year, Roche Pharmaceuticals was also on board to shepherd the drug through clinical trials. After its 2009 acquisition of Genentech, Roche moved the project to Genentech.
From the outset, preclinical data indicated that the drug wouldn’t work for patients without the BRAF mutation, says Christopher Bowden, vice president of product development at Genentech. Roche started using a prototype BRAF mutation test early in the Phase I trials, and by the time Phase II testing was initiated, the near-final version of the test was already being used for patient selection.
Selecting those patients speeded up the clinical trials and reduced the number of patients required to show a therapeutic benefit. The Phase I results were so dramatic that the definitive Phase III trial was initiated even before the Phase II trial was finished, Koch says. Likewise, on the basis of the impressive Phase II results, the Phase III study was analyzed early, and upon the advice of an independent data-monitoring board, the study results were released. At that point, patients in the control arm of the trial were allowed to cross over to the treatment arm to benefit from the medication.
The drug and diagnostic development timelines were coordinated closely enough that both applications could be submitted to FDA together. “FDA has been nothing but supportive of this process and did its absolute best to help us coordinate the regulatory filings,” Koch says. The team submitted the applications in a modular fashion, which allowed FDA to review some data early. Roche filed the completed applications for the drug and the diagnostic in April 2011, and both were approved on Aug. 17, 2011, ahead of schedule.
Thanks to a companion diagnostic, Pfizer also was able to accelerate the timeline for Xalkori as a treatment for non-small-cell lung cancer. Pfizer was already testing the drug for cancers driven by the c-Met oncogene. Researchers knew that the drug could target the ALK (anaplastic lymphoma kinase) gene as well, but they thought ALK was involved only in non-Hodgkin’s lymphoma. In 2007, rearrangements of the ALK gene were found to drive a small segment of lung cancers as well. Pfizer quickly shifted gears to focus on non-small-cell lung cancer.
From discussions with FDA, Pfizer knew it would need a test to identify the right patients. “We looked at the different options,” Buller says. The possible assay technologies included polymerase chain reaction, immunohistochemistry, and fluorescence in situ hybridization (FISH). “Because a number of major institutions in the U.S. that were enrolling patients in the trial were using the Abbott Vysis [FISH] probes, it seemed most logical to continue along that line,” Buller says. Abbott Laboratories’ FISH method uses fluorescent probes to detect particular DNA sequences on chromosomes.
“Since Abbott already had an ALK probe on the market, Pfizer approached us, seeking the development of a test that could determine an individual’s genetic status for use in selecting patients for its crizotinib clinical trials,” says Stafford O’Kelly, president of Abbott Molecular.
In 2009, Pfizer and Abbott entered into a development and commercialization agreement for ALK FISH probes. Abbott modified its existing ALK probes, which had been designed for blood samples, to create a diagnostic test optimized for non-small-cell lung cancer tissue, ensuring no patients with the ALK gene rearrangements are missed.
By using the test to identify patients, Pfizer scientists were able to focus the trials so that the therapeutic effect was readily apparent. “The magnitude of the clinical benefit was so dramatic that the approval occurred without Phase III clinical data,” Buller says. The two trials had 119 patients in one and 136 in the other, and neither trial had a comparator arm. A typical lung cancer drug approval would have required a Phase III trial with 500 to 900 patients prior to approval. Even with the accelerated approval, FDA required Pfizer to continue Phase III trials, which were already under way. The entire process—from discovery of ALK’s lung cancer connection to regulatory approval—took about four years.
FDA was a key partner in the process, Buller says. “This isn’t something where we went once, talked to FDA, and came back in two years with the package,” he says. “It was a tremendous partnership.”
The agency is spending lots of time helping companies navigate the process, FDA’s Mansfield says. “We try to address any problems we see well before they’ve submitted an application,” she says.
FDA specified the requirement to use diagnostics in the drug labels; physicians must use an FDA-approved test before prescribing these drugs. For both Zelboraf and Xalkori, the options boil down to the tests developed and validated in parallel with the therapeutic. Pfizer is working with Ventana Medical Systems, a Roche company, to develop a second test, this one based on antibodies, to identify patients who can receive Xalkori.
An FDA-approved test “will have gone through our scrutiny and really been pushed to its limits,” Mansfield says. “We know exactly how it performs. When you develop a test and you don’t use the patient samples from the clinical trials and nobody’s taken a look at your data to see how well it performs, I think you stand a good chance of getting differences in test results that might not be good for patients.”

Furthermore, companion diagnostics need to meet all the regulatory criteria FDA sets for any stand-alone test. “People are starting to realize that companion diagnostics are not just biomarkers or research tools,” says Ron Mazumder, global head of research and product development at Janssen Diagnostics, part of the Janssen Pharmaceuticals unit of Johnson & Johnson. “They are in fact regulated, commercialized tests. It’s really important to think about not only the technology and the biomarker itself, but the regulatory path and commercialization obstacles.”
The Zelboraf and Xalkori collaborations highlight two models for partnerships to develop such diagnostics. For Genentech and Roche Molecular Systems, the collaborators being part of the same company made the process go more smoothly than working with outside partners. “I had somebody on the biomarker team from day one as development started,” Koch says. Because drugs and diagnostics are such different businesses, being involved from the start “leads to much greater shared understanding and appreciation of what’s needed.” Problems that arise can be resolved quickly, he says.
External partnerships work too but take extra effort. “Early on in the collaboration, we established an organizational structure and a process to ensure that both companies were communicating effectively,” Abbott’s O’Kelly says of Abbott and Pfizer’s cooperation on the ALK test for Xalkori patients. “Through this organizational structure, we were able to coordinate the required timelines, which were extremely ambitious.”
“There weren’t any obstacles we couldn’t overcome,” Buller says. Both companies were motivated to get the combination to patients as quickly as possible.
“We learned that close collaboration and communication will be key in adapting successfully to this shift toward more personalized treatments,” O’Kelly says. “No one company or entity has all the answers—a variety of expertise and experience is required.”
Most companion diagnostics so far have been for cancer and HIV. But companies are working on drug/test combos in other therapeutic areas, including neurological, autoimmune, inflammatory, and cardiovascular diseases. And those that don’t yet have drug/diagnostic pairs are getting in on the act.
Johnson & Johnson is implementing a “beyond-the-pill paradigm,” Mazumder says, to combine diagnostic information with pharmaceuticals. The center he heads, he says, is “charged as acting as a centralized resource” for all therapeutic areas. The company currently has a total of nine companion diagnostics programs in oncology, neurology, and infectious and cardiovascular diseases.
\

\
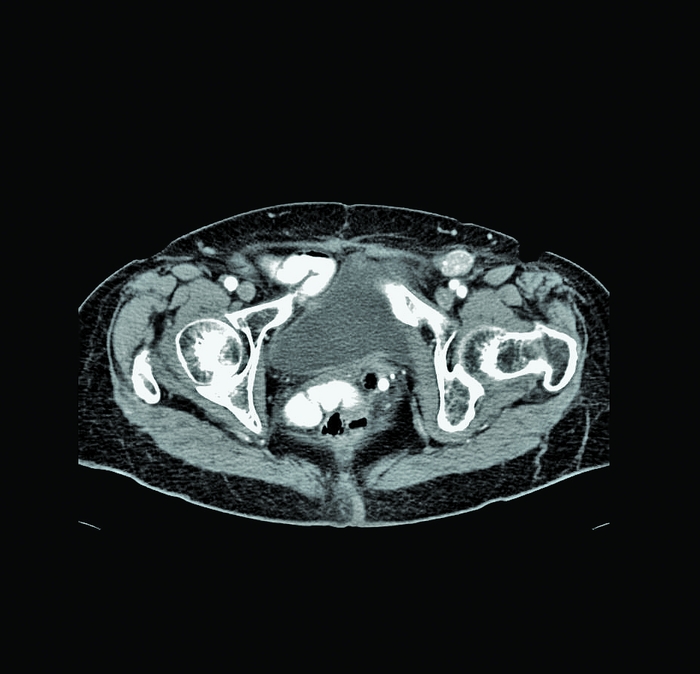
Physicians can use a combination of a computed tomography scan (top) and an image of folate receptors to determine if a patient is a candidate for Endocyte’s targeted therapy. These images show the pelvis of a patient with ovarian cancer. In the bottom image, the black circle is the ovarian tumor; the larger black area is the bladder.
UCB Pharma, based in Belgium, is looking for ways to stratify patient populations in rheumatoid arthritis, according to Duncan McHale, vice president of global exploratory development. At this point, however, no biomarker at UCB has risen to the level of a companion diagnostic, he notes.
The biopharmaceutical company Endocyte is built on the idea of companion diagnostics, says Ron Ellis, president and chief executive officer. The company develops conjugates of small-molecule drugs, consisting of an extremely potent therapeutic agent—so potent it can’t be administered without targeting—covalently linked to a targeting agent, the vitamin folate. Folate leads the tethered drug to folate receptors on a cell’s surface. Such receptors are found only on rapidly dividing cells such as developing fetuses or cancer cells. Being able to identify patients with folate receptors and the locations of those receptors is crucial to prescribing the treatment only for patients who are likely to respond.
That’s where companion diagnostics come in. The same folate that guides the drug can also ferry imaging agents to the receptors.
Advertisement
“We just take off the drug and add an imaging agent but leave the targeting ligand,” Ellis says. “We can look at all the cancer or target lesions and understand the presence of the receptor” throughout the body.
The imaging agent consists of folate linked to a radioactive isotope of technetium. Radiologists inject the agent into a patient; an hour later they use a gamma camera to detect radiation from the technetium. The diagnostic can be used immediately before treatment to make sure the receptors really are there.
Endocyte is developing its lead drug, vintafolide, which targets platinum-resistant ovarian cancer, in partnership with Merck & Co. “These patients have never had a drug that delays disease progression,” Ellis says. In Phase II trials, Endocyte’s drug has shown a statistically significant ability to delay disease progression, Ellis says. “How have we been able to see this when other drugs haven’t?” he asks. “We’re picking the right patients with the diagnostic, and we’re delivering a highly targeted therapy.”
Vintafolide is currently in Phase III clinical trials, which should be finished in early 2014, Ellis says. The company hopes to win conditional approval in Europe next year. It should be able to submit clinical data to FDA in 2014. Endocyte is also exploring use of vintafolide in other indications including non-small-cell lung cancer by selecting patients with the same companion imaging diagnostic.
The diagnostic could be used for any drug that targets the folate receptor, Ellis says. No approved drugs target that receptor, but some drugs currently in clinical trials do.
A few companion diagnostic tests have been developed for drugs that are already on the market. For example, a genetic test that looks for variants in two genes was developed to guide doctors in identifying patients who would be at risk of uncontrolled bleeding if given the anticoagulant warfarin. But insurance companies have been reluctant to pay for the test, and Medicare has gone so far as to refuse to pay for it. Because these tests aren’t required for the safe and effective use of the drug, they aren’t considered to be companion diagnostics in FDA parlance.
In that case, the main problem is that the test doesn’t tell physicians what they need to do, says Joshua P. Cohen, a health economist at Tufts Center for the Study of Drug Development who has studied market access to personalized medicine. It tells them which patients are at risk for uncontrolled bleeding, he adds, but it doesn’t tell them what dose they should prescribe.
Yet when Medco Research Institute studied the clinical utility of the warfarin markers, “we were able to demonstrate a 30% reduction in hospitalization,” says Felix W. Frueh, president of the institute. “That’s dramatic.” But he notes the continuing opposition to the test.
Frueh also notes that “when a drug is already on the market, who has incentive to put forth millions to study a novel marker and how it impacts that therapy?” Academic researchers are more likely than companies to undertake such studies, he says.
“You probably won’t see a complete and dramatic shift in the way drugs are being used once they’re on the market,” Frueh says. Companion diagnostic studies are easier if done during drug development and prior to marketing.
Personalized medicine and companion diagnostics appear to be the way forward for drugs yet to be developed. Roche and Pfizer, both of which have had drugs approved under the pathway set up by FDA’s guidance document, see companion diagnostics as a significant part of their future. Roche has set a goal of making sure at least half its drugs in early development have a companion diagnostic. “We’re seriously committed to personalized health care,” Hampton says.
At Pfizer, the Xalkori experience has led to the formation of a company-wide companion diagnostics group to move the concept beyond oncology, Buller says. “While companion diagnostics aren’t going to be perfect for every drug, we want a significant portion of our portfolio to move forward on the basis of diagnostic testing.” Ideally, diagnostics would be planned from the start of development, but it’s essential to retain the flexibility to change the selection strategy in response to gene discoveries made after a drug’s already in the clinic, he notes.
“The landscape and behaviors that will allow personalized medicine to flourish are just beginning to take shape,” O’Kelly says. “The emergence of companion diagnostics will continue to change how diagnostics and pharmaceutical companies collaborate during the discovery and development phases. We’re already seeing an increasing number of tests being developed in combination with—rather than separate from—the drugs with which they will be used.”
You might also like...


The power is now in your (nitrile gloved) hands
Sign up for a free account to get more articles. Or choose the ACS option that’s right for you.
Already have an ACS ID? Log in
Join the conversation
Contact the reporter
Submit a Letter to the Editor for publication
Engage with us on Twitter