Advertisement
Grab your lab coat. Let's get started
Welcome!
Welcome!
Create an account below to get 6 C&EN articles per month, receive newsletters and more - all free.
It seems this is your first time logging in online. Please enter the following information to continue.
As an ACS member you automatically get access to this site. All we need is few more details to create your reading experience.
Not you? Sign in with a different account.
Not you? Sign in with a different account.
ERROR 1
ERROR 1
ERROR 2
ERROR 2
ERROR 2
ERROR 2
ERROR 2
Password and Confirm password must match.
If you have an ACS member number, please enter it here so we can link this account to your membership. (optional)
ERROR 2
ACS values your privacy. By submitting your information, you are gaining access to C&EN and subscribing to our weekly newsletter. We use the information you provide to make your reading experience better, and we will never sell your data to third party members.
Biological Chemistry
Patrick McNutt Talks Chemical Weapons
Army scientist discusses medical research being carried out to understand and protect against warfare agents
by Sarah Everts
April 20, 2015
| A version of this story appeared in
Volume 93, Issue 16

Just four days after defending a Ph.D. in molecular biology at Princeton University, Patrick McNutt started basic infantry training at Fort Benning, Ga. “That led to some culture shock,” he recalls with a chuckle. But the experience prepared him to deploy in 2005–06 to Iraq, where he provided science and technology ground support as a member of the Reserve Officers’ Training Corps, a military program that financially supported the bachelor’s degree he received from Wake Forest University.
Today, McNutt, who clearly doesn’t relish a humdrum life, works for the U.S. Army Medical Research Institute of Chemical Defense (USAMRICD), the primary laboratory of the Department of Defense for investigating medical aspects of chemical weapons defense. He studies the biological and biochemical mechanisms of nerve agents, mustard gas, and botulinum neurotoxins. What follows is a recent discussion (edited for length and clarity) he had with C&EN about why chemical weapons defense research is relevant today.
With the Chemical Weapons Convention (CWC) in place, do we really need chemical defense research?
Chemical warfare agents are widely available, inexpensive, and don’t require an extensive educational background to produce. Many of them are relatively simple to synthesize. In fact, there are pesticides out there, albeit far less potent, that act similarly to traditional nerve agents.
This week in 1915, the German Army released chlorine gas on Allied troops at Flanders Fields, in Belgium. Learn more about this first use of chemicals as weapons of mass destruction at http://chemicalweapons.cenmag.org.
With the CWC in place, state-sponsored production, storage, and distribution of chemical weapons is being eliminated. Although we have probably gotten rid of the majority of state-sponsored risk, we are still at risk from individual actors—from lone wolves.
So individuals are still a threat. What do we know about the chemical agents they might use?
To a first-order approximation, we know how the vast majority of these agents work in the body. Traditional nerve agents block acetylcholinesterase activity, preventing the breakdown of the neurotransmitter acetylcholine. Mustard gas forms adducts that lead to genotoxicity (DNA damage), to inappropriate cellular signaling, and to interference with protein-based biochemistry. Botulinum gets into the presynaptic nerve terminal and cleaves proteins required for neurotransmitter release. Ricin blocks protein synthesis. All of these we generally understand and can replicate with cells in a dish.
If someone experiences a chemical weapons attack, what can be done by first responders to mitigate damage?
With the majority of chemical warfare agents, the time frame in which you need to apply a treatment after exposure is very, very short—minutes, in many cases. Unless you can eliminate the agent before it hits its biological target, there’s often not much you can do to mitigate the severity of the injury.
Cyanide chelators such as hydroxocobalamin are under experimentation. For mustard, the most important response is physical decontamination. Wash the exposed surface as fast as you can with a mild detergent; most mustard exposure is through the skin. However, if you inhale it … that requires an immense amount of medical support.
For nerve agents, there are oximes, which knock the nerve agent off of acetylcholinesterase, reactivating the enzyme. And there are protein bioscavengers under development that can help find and remove nerve agents from the bloodstream. The key to their use—and they are not battlefield tested yet or approved by the National Institutes of Health—is going to be delivering them at sufficient concentrations and fast enough.
What are some of the big unanswered questions in chemical weapons defense?
We understand the biochemical mechanism of most of these agents. It’s the long-term biological consequences of the initial biochemical reactions where research is very much needed. In my opinion, that’s where the most effective treatments are going to come from. You have a short window of time after exposure to interfere with the biochemical actions of chemical agents, but then you may have days, months, years, decades to manage the long-term consequences of exposure among survivors.
If you review the medical accounts of survivors of the sarin attacks in the Tokyo subway, among those that had seizures and survived, the vast majority exhibited a range of neuropsychiatric changes in the long term.
You have approximately 1011 neurons in your central nervous system that form 1014 synapses (nerve junctions). What we’ve found is that, in the amygdala (which controls impulsivity) and the hippocampus (which controls certain types of memory and learning), the function of synapses becomes altered when the brain seizes from nerve agent exposure. Thus, when nerve agents block acetylcholinesterase function in the central nervous system, it triggers a massive change in circuit function. But how that circuit function disruption results in these long-term neuropsychiatric deficits and how to reverse it, these are some of the interesting questions.
When soldiers are exposed to a suspected chemical weapon, what are they supposed to do?
You get into what’s called a military-oriented protective posture: It’s effectively a suit with a gas mask, gloves, and everything else. You get in that suit as fast as you can. Then some field tools are deployed: detection systems that can in some cases identify what agents are present. And then you are going to evacuate that area as fast as you can, ideally to a decontamination facility set up outside of the exposure zone. There, you’ll be decontaminated, you’ll discard your protective gear, and you’ll go directly into a medical facility to be checked out.
That’s for military. What options do civilians have?
There’s a paper from 2014 in the Annals of Internal Medicine about lessons learned from the Syrian sarin attack (DOI: 10.7326/m13-2799). These researchers went on YouTube and found all the uploaded videos from the attack. They used the videos to track the implementation of medical countermeasures, the symptoms that casualties developed, et cetera. It is a great—and I don’t mean “great” in a good way—example of the type of chaos caused by a civilian population being exposed to warfare agents and how overwhelmed the medical response may be. To be honest, your first responders are probably not going to be well trained in how to treat a civilian chemical warfare attack. It’s something they don’t see often. To keep people alive who have been severely exposed … well, even if you have some sort of treatment to keep them alive, they require a lot of personal, one-on-one work. In field conditions, or even in the trauma unit of a hospital, my concern is that the medical support teams are going to be overwhelmed quickly.
What do you do to keep yourself safe in the lab?
We work with mustard, we work with nerve agents, and we work with botulinum. As frustrating as it is to have our safety office constantly hovering over us, they do a phenomenal job to make sure we do everything possible to minimize all risks. We have engineering controls, a lot of personal training, and the appropriate personal protective equipment: gloves, masks, gowns. People feel more at risk from our safety people yelling at us than from the chemicals themselves.
Where should the field of chemical weapons defense be heading?
In my opinion, there should be increased emphasis on the biological responses to chemical weapons as opposed to their biochemistry. Pragmatically, in civilian exposures, and most likely in military ones, there’s not a lot we are going to be able to do to prevent these agents from exerting their effect on people. They work too fast, they are too potent—that’s why they are so effective. At this point, I think the focus needs to be on improving acute care to increase the probability of survival and help survivors recover from the damage that’s been done.
WEAPONIZED How the two biggest chemical weapons threats stack up
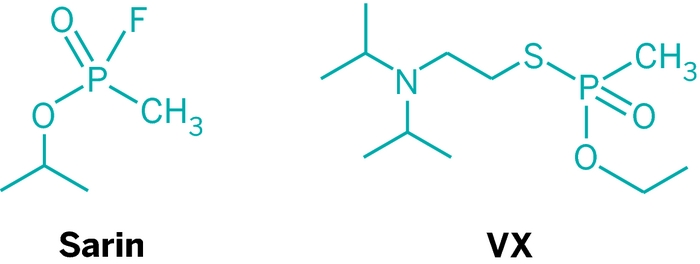
NERVE AGENTS

Credit: Noboru Hashimoto/Sygma/Corbis
Infamous deployment: In 1995, a religious cult released sarin on the Tokyo subway (shown), killing 12 people and injuring thousands. In 2013, hundreds of Syrian civilians were killed by the government’s use of sarin.
Exposure symptoms: Eye irritation, dilation of pupils, shortness of breath, intense sweating, vomiting, muscle twitching, seizures, loss of consciousness, and asphyxiation.
Biological mechanism: Nerve agents block the activity of acetylcholinesterase so it cannot break down the neurotransmitter acetylcholine. Muscle and other organ cells that receive signals from acetylcholine-emitting nerve cells become overstimulated.
First response: Atropine helps calm overstimulated cells. Pralidoxime and other oxime compounds kick nerve agents off acetylcholinesterase.
Long-term effects of exposure: Cognitive and memory dysfunction, aggression, and difficulty processing emotions.
On the horizon: Protein scavengers for nerve agents based on two human proteins—butyrylcholinesterase and paraoxonase—that can bind and trap nerve agents.
SOURCES: Organisation for the Prohibition of Chemical Weapons, USAMRICD, Patrick McNutt
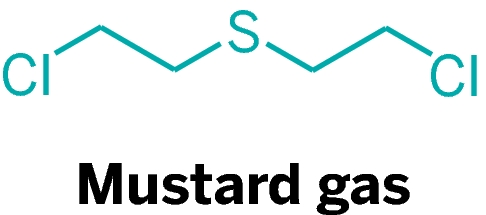
Blistering agent: Mustard gas

Credit: Associated Press
Infamous deployment: Known as the “king of the battle gases,” mustard was first deployed by the German Army in 1917 and then adopted by the Allies. It was also used during the Iran-Iraq War in the 1980s (shown).
Exposure symptoms: Initially nothing. Then two to 48 hours after exposure, extensive, painful blisters form, which can lead to infection and sepsis. Skin and organ inflammation. Uncontrollable tearing, sensitivity to light, and nausea and vomiting.
Biological mechanism: Mustard is an alkylating agent that forms adducts with DNA bases. Mustard also binds glutathione, preventing this small-peptide antioxidant from doing its important job of sweeping up free radicals created during cell respiration. The consequence is severe tissue damage.
First response: Washing with detergent can remove mustard gas. Prophylactic anti-inflammatory drugs and antibiotics treat symptoms.
Long-term effects: Blindness, damage to the lungs and respiratory tract, and increased vulnerability to chronic lung diseases.
On the horizon: Organ-specific treatments based on controlling acute inflammatory responses. Treatments to accelerate tissue regeneration.
SOURCES: Organisation for the Prohibition of Chemical Weapons, USAMRICD, Patrick McNutt
Chemical & Engineering News
ISSN 0009-2347
Copyright © 2024 American Chemical Society
You might also like...


The power is now in your (nitrile gloved) hands
Sign up for a free account to get more articles. Or choose the ACS option that’s right for you.
Already have an ACS ID? Log in
Join the conversation
Contact the reporter
Submit a Letter to the Editor for publication
Engage with us on Twitter