If you have an ACS member number, please enter it here so we can link this account to your membership. (optional)
ERROR 2
ACS values your privacy. By submitting your information, you are gaining access to C&EN and subscribing to our weekly newsletter. We use the information you provide to make your reading experience better, and we will never sell your data to third party members.
For drugmakers, the year opened with uncertainty about an unconventional new Administration in Washington. The industry braced itself for public scrutiny, and it came swiftly in the form of President Donald J. Trump’s barbed remarks in press conferences and on Twitter about the high price of drugs and how he will rein them in.
So far, those promises have been empty, but the focus on the high cost of health care isn’t going away. Every few months of 2017 brought a new face of drug industry greed. Under new leadership, the U.S. Food & Drug Administration began to make it harder for bad actors to keep prices on old drugs high.
Despite the pressure on cost, the industry had many moments to shine in 2017. The first genetically engineered T-cell therapies were approved, and a gene therapy is on the cusp of reaching people with a rare form of blindness.
Moreover, the year brought yet another new crop of well-funded companies working on the edges of technology—next-generation cellular therapies, the gene-editing technology CRISPR, and other tools in search of the next wave of therapeutic advances.
Advertisement
Pharma navigates a new Administration
Empty threats and promises from Trump left drugmakers grappling with uncertainty
Trump had a friendly meeting with pharmaceutical executives at the start of the year but has been adversarial on social media.
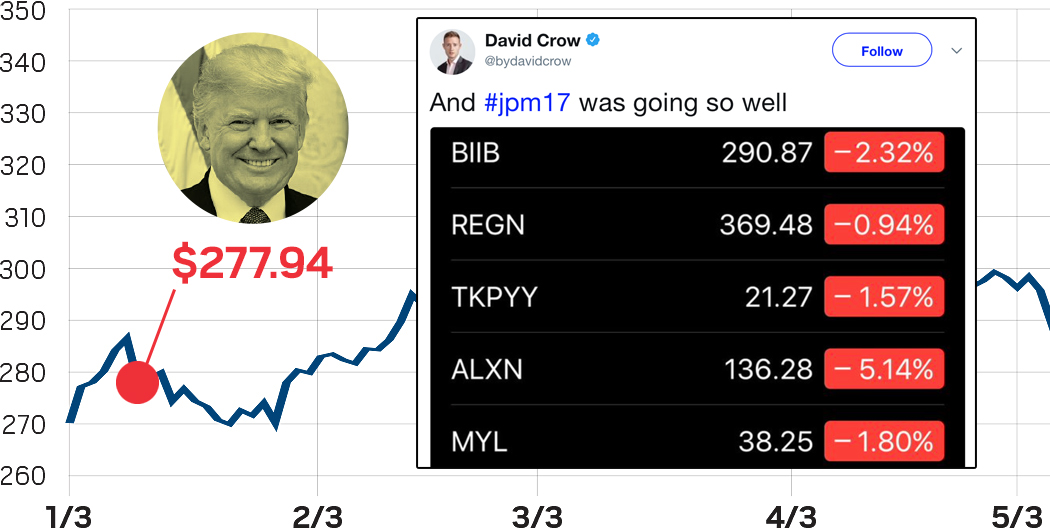
It was a sound bite that reverberated through the drug industry. On Jan. 11, in his first news conference as president-elect, Donald J. Trump castigated pharmaceutical companies as “getting away with murder.” In the next breath, he vowed to shake up how the government paid for drugs.
Those 29 seconds of commentary sent the biotech stock index down 3%. It would become just one of many off-the-cuff remarks directed at the pharmaceutical industry in Trump’s first year in office.
The price negotiation threat has so far turned out to lack teeth. But the general uncertainty around key issues in the Trump agenda—the fate of health care reform, corporate tax reform, even the ability to bring talented foreign scientists to the U.S.—has left companies and investors on edge.
For investors, the uncertainty wrought by Trump poses a challenge. “In a world where an Administration is more unpredictable, that’s a net negative for many of us,” says Bruce Booth, a partner at life sciences-focused Atlas Venture. “We prefer clear policy agenda items, clear choices, and therefore things we can evaluate in our scenario planning for the next three to five years. We would all benefit from an Administration who is more consistent, more predictable, more measured in the way that it approaches these subjects.”
The failed attempt to push health care reform through Congress ate up much of the agenda for the new Administration, leaving little progress on the one issue that drug industry watchers agree would markedly affect pharma companies in 2018: tax reform.
The high corporate tax rate in the U.S. has caused many companies to park substantial cash overseas—$150 billion, Ernst & Young estimates. Until a 2016 Treasury Department rule made it more difficult, the high taxes even prompted some companies to acquire overseas firms in order to shift their headquarters to countries with more favorable tax codes.
Trump has proposed a law that would encourage companies to repatriate, or bring back, that overseas money, a possibility that many in the industry say could spur big pharma firms to do more deals. Merger and acquisition activity was modest in 2017.
“If we allow for repatriation at a lower rate of 10 to 15%, some good things could come out of it because a lot of money is sitting outside the U.S.,” says Ambar Boodhoo, Americas transactions services life sciences leader at Ernst & Young. “I’m hoping they don’t take the cash and just start buying back shares and paying dividends.”
CAR-T cancer immunotherapy took off
Two personalized immune-cell therapies came to the market, and more are likely on the way
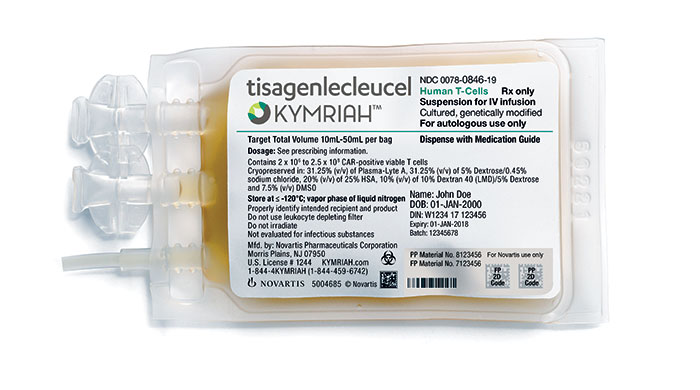
An IV bag of Kymriah, the one-time, $475,000 CAR-T immunotherapy treatment from Novartis, contains a patient’s genetically engineered T cells.
In a sweeping success for cancer immunotherapy this year, the U.S. Food & Drug Administration approved the first two treatments that use a patient’s own genetically engineered cells to combat specific kinds of blood cancer.
Both new drugs are CAR T-cell immunotherapies, created by injecting an individual’s T cells with DNA that encodes a chimeric antigen receptor (CAR). The CAR proteins jut from the immune cells’ surfaces and direct them to seek and destroy tumor cells.
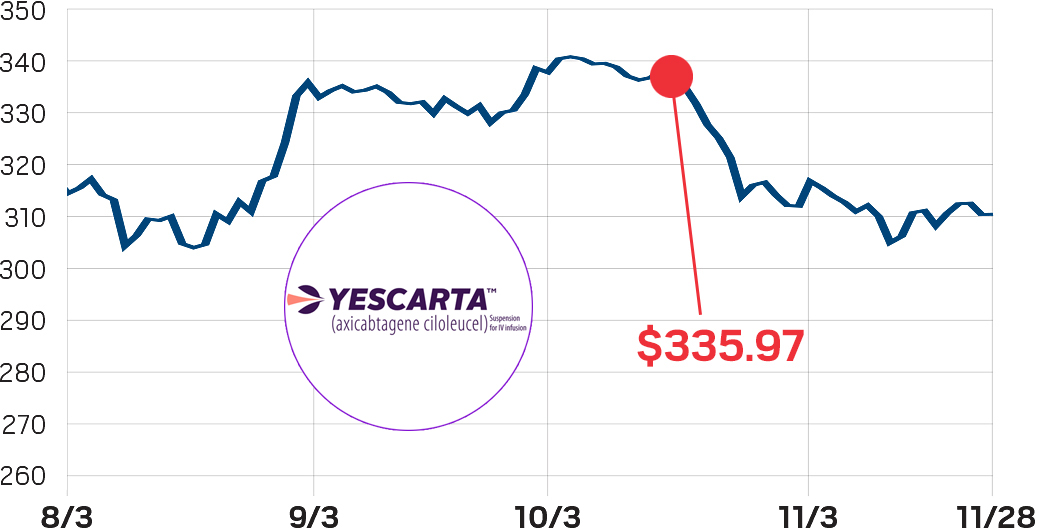
Some 83% of people treated with the first approved CAR-T drug, Kymriah from Novartis, achieved complete remission—no cancer detected—within three months. More than 50% of people treated with the second drug, Kite Pharma’s Yescarta, are in complete remission.
“The excitement is justified; it is a validation of the field,” says David Epstein, former CEO of Novartis Pharmaceuticals.
Despite the excitement, many challenges remain for CAR-T therapies. To start, both treatments were approved for a small subset of cancers.
Kymriah treats people up to 25 years old who have acute lymphoblastic leukemia of B-cell origin who are resistant to treatment or have relapsed twice, limiting potential patients to a few hundred per year. Yescarta treats large B-cell lymphoma in adults after two other treatments have failed. It could help an estimated 7,500 people per year.
“The number one challenge for CAR-T is to get it to work more broadly,” says Brad Loncar, a biotech investor specializing in immunotherapy. If CAR-T therapy ends up being useful for only a few kinds of cancer, “it will be a huge failure,” although Loncar thinks this scenario is unlikely.
One company to watch is Bluebird Bio, which recently announced promising Phase I clinical trial data using a different kind of CAR-T therapy to treat multiple myeloma. But even if CAR-T works for other blood cancers, applying the technique to the majority of solid tumors will be difficult.
Loncar says the CAR-T company “the market is most excited about” is Juno Therapeutics, which has more than 10 clinical programs for blood and solid tumors. Juno’s most advanced program fell behind after five patients died from CAR-T-induced brain swelling.
Toxicity is a lingering issue for other CAR-T therapies too. Kymriah and Yescarta both come with warnings for cytokine release syndrome, a severe, body-wide immune reaction after injection of the drug. “It’s not an exaggeration to say that it almost kills you before it helps you,” Loncar says.
The personalized nature of CAR-T makes manufacturing another complication. Some companies, including Cellectis, are designing “off-the-shelf” CAR-T cell therapies made ahead of time with other people’s cells.
Pricing, however, is perhaps the issue that’s most captured the public’s attention. The drug industry has signaled that CAR-T will be a big business. Less than two months before Yescarta’s approval, Gilead Sciences acquired Kite Pharma for $11.9 billion.
Kymriah’s one-time cost of $475,000 and Yescarta’s price tag of $373,000 caused sticker shock and spurred broader questions about the affordability of CAR-T and gene-therapy treatments. Novartis said people won’t pay for Kymriah if they don’t respond to treatment within a month.
“CAR-T is not expensive because of greed,” Loncar says. It is expensive because of the logistics, limited patient population, and its novelty, he adds. “CAR-T is state of the art, and this is just the beginning.”
A whirlwind year for the drug industry
Against the backdrop of a rising biotech stock index, the pharmaceutical industry in 2017 juggled an unpredictable new Administration, breathtaking technological advances, modest deal-making, and the never ending conversation about drug prices
Ipsen kicks off year with $1 billion purchase of Merrimack Pharmaceuticals
Credit: Ipsen
iShares Nasdaq biotech stock index ($)
1/9/17
Takeda pays $5.1 billion for cancer-focused Ariad Pharmaceuticals
Credit: Takeda
iShares Nasdaq biotech stock index ($)
1/11/17
President Trump says in a press conference that drug companies are “getting away with murder,” sending stocks tumbling
Credit: Wikimedia Commons
iShares Nasdaq biotech stock index ($)
1/23/17
The trade association PhRMA unveils a PR campaign aimed at improving the drug industry’s image
Credit: Youtube
iShares Nasdaq biotech stock index ($)
1/31/17
President Trump meets with pharmaceutical executives, promising to speed up drug approvals and cut regulations
iShares Nasdaq biotech stock index ($)
2/10/17
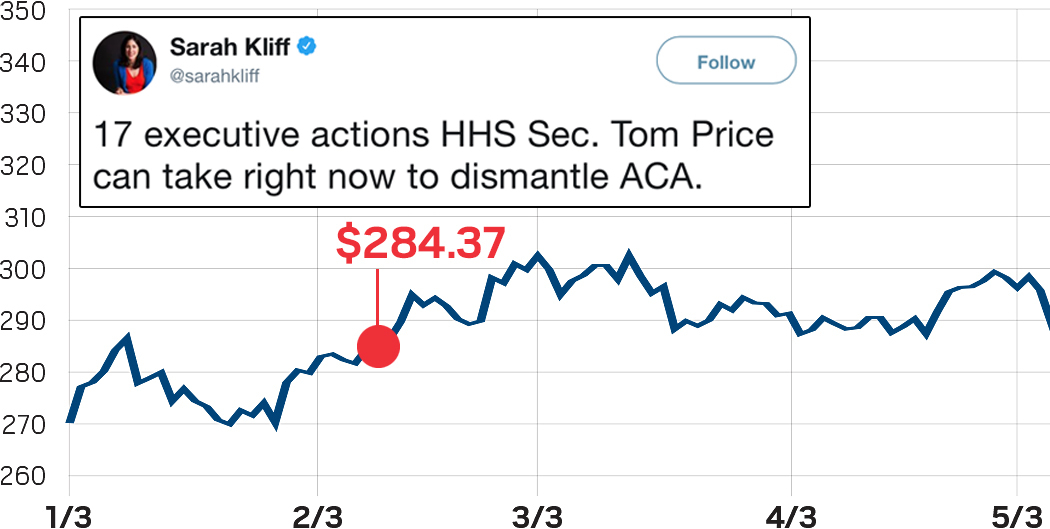
Tom Price is confirmed as Health & Human Services secretary
iShares Nasdaq biotech stock index ($)
2/13/17
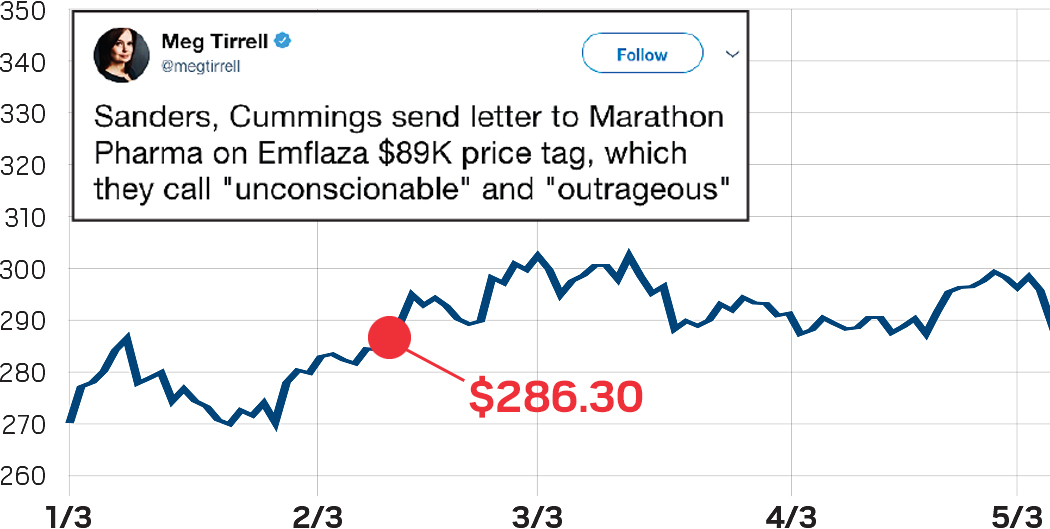
Days after getting FDA approval for a steroid for Duchenne muscular dystrophy, Marathon Pharmaceuticals became the latest face of drug price gouging
iShares Nasdaq biotech stock index ($)
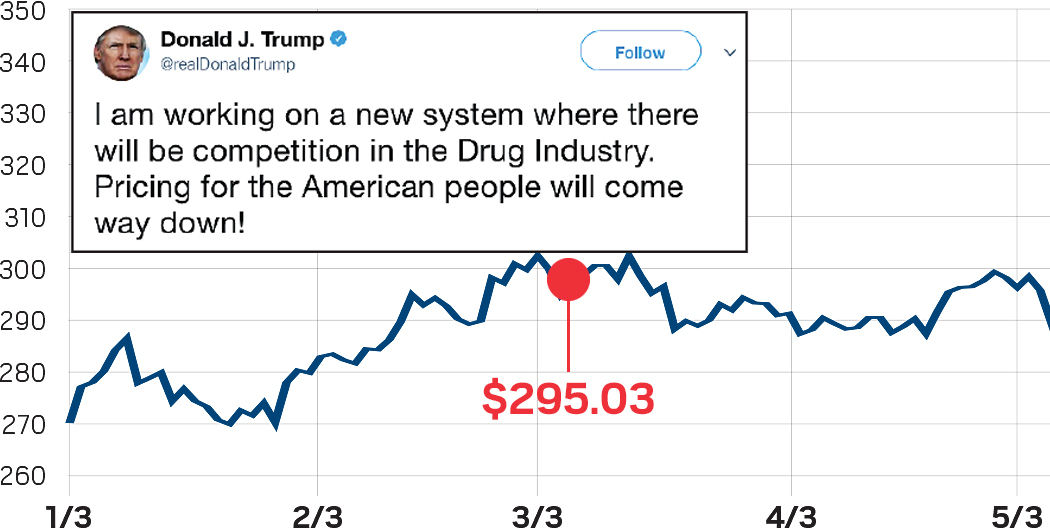
3/7/17
Trump claims to be working on drug pricing
iShares Nasdaq biotech stock index ($)
3/22/17
March for Science takes place in cities across the globe, and some biotech companies take part
Credit: Jyllian Kemsley/CE&N
iShares Nasdaq biotech stock index ($)
3/24/17
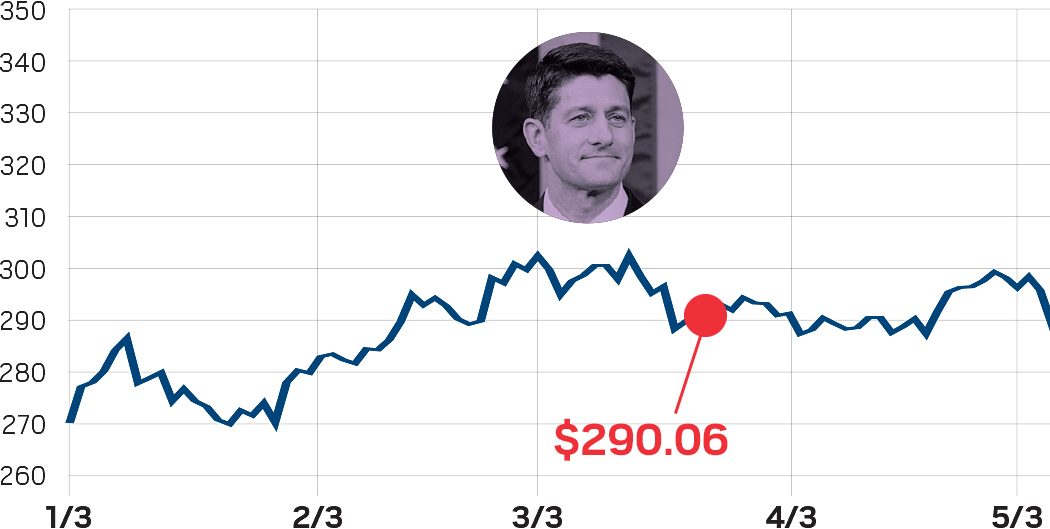
Led by Paul Ryan, Republicans withdrew their bill to repeal the Affordable Care Act
Credit: Wikimedia Commons
iShares Nasdaq biotech stock index ($)
4/3/17
Emma Walmsley officially takes over as CEO at GlaxoSmithKline, becoming the first woman to lead a big pharma firm
Credit: Walmsley
iShares Nasdaq biotech stock index ($)
5/9/17
Scott Gottlieb confirmed as head of FDA
Credit: Wikimedia Commons
iShares Nasdaq biotech stock index ($)
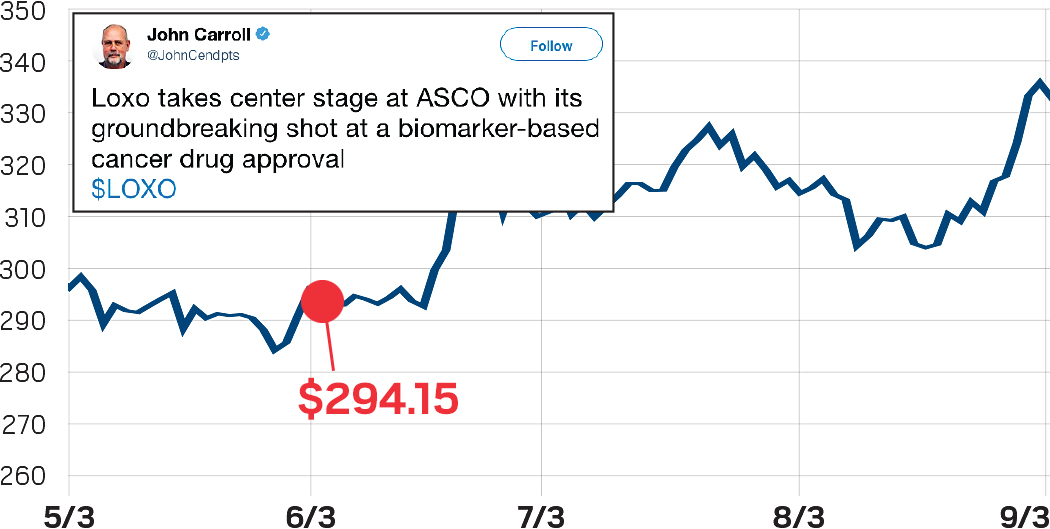
6/5/17
Data from Loxo Oncology’s TRK inhibitor larotrectinib grabs the spotlight at the American Society of Clinical Oncology meeting
iShares Nasdaq biotech stock index ($)
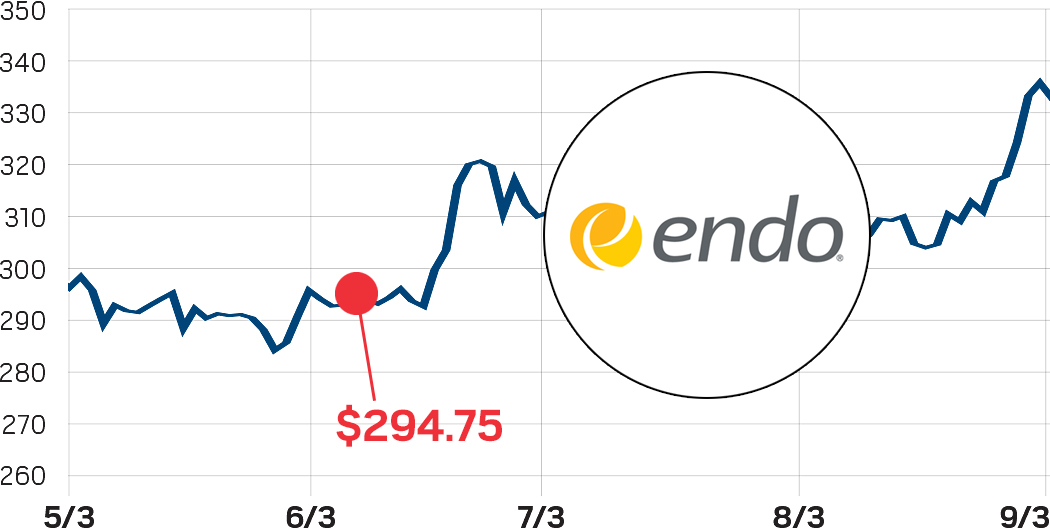
6/8/17
FDA asks Endo Pharmaceuticals to take its long-acting opioid, Opana ER, off the market, saying risks of abuse outweigh the drugs benefits
Credit: Endo Pharmaceuticals
iShares Nasdaq biotech stock index ($)
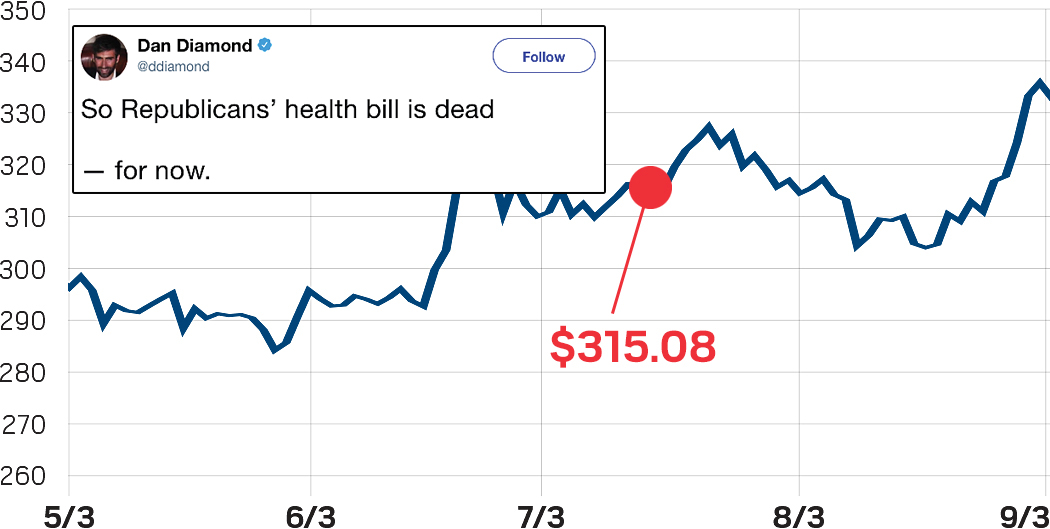
7/17/17
Republican health bill dies
iShares Nasdaq biotech stock index ($)
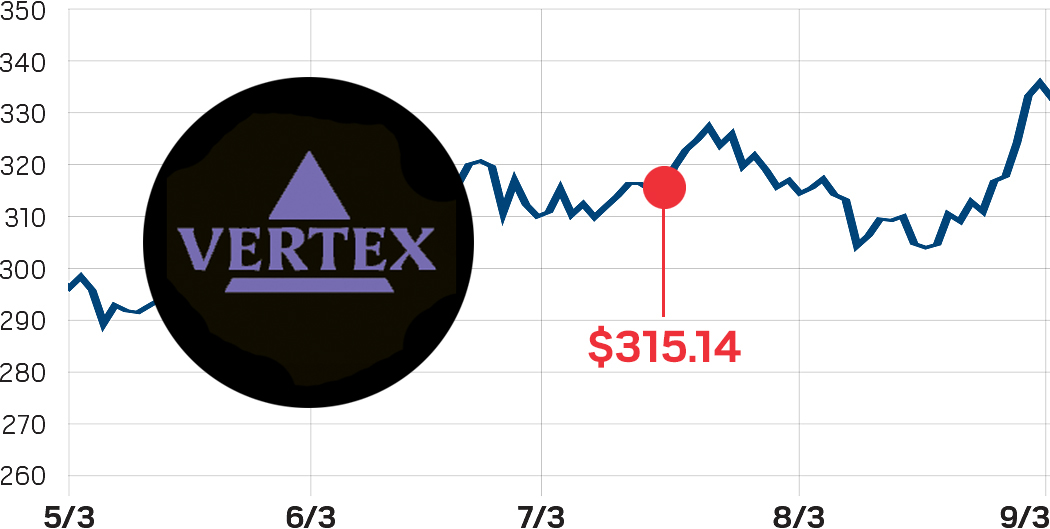
7/18/17
A three-drug combo from Vertex Pharmaceuticals improves lung function in people with cystic fibrosis, potentially expanding treatment to 90% of patients
Credit: Vertex Pharmaceuticals
iShares Nasdaq biotech stock index ($)
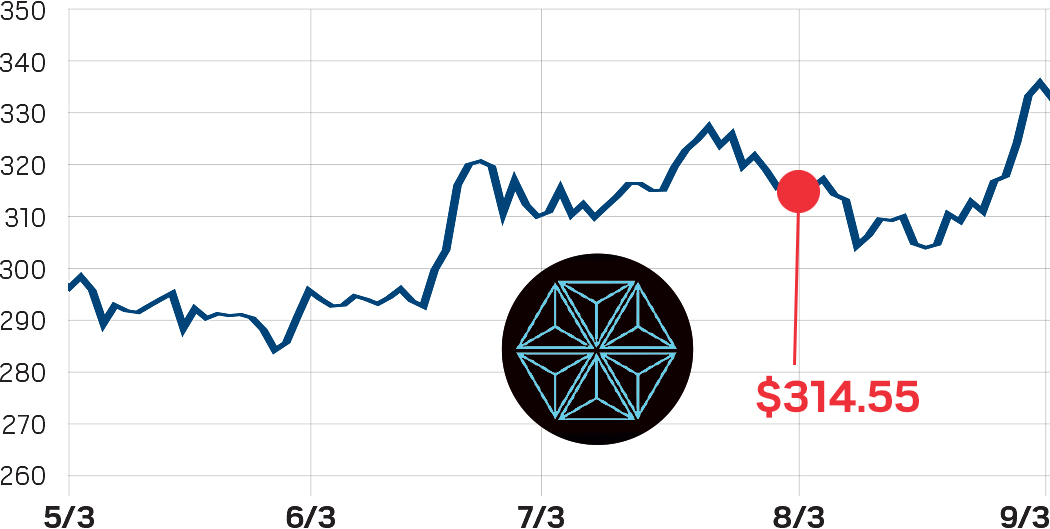
7/24/17
Mitsubishi Tanabe pays $1.1 billion for neuroscience-focused NeuroDerm
Credit: Mitsubishi Tanabe
iShares Nasdaq biotech stock index ($)
8/3/17
Bristol-Myers Squibb pays up to $2.3 billion for immunology-focused IFM Therapeutics
Credit: Bristol-Myers Squibb
iShares Nasdaq biotech stock index ($)
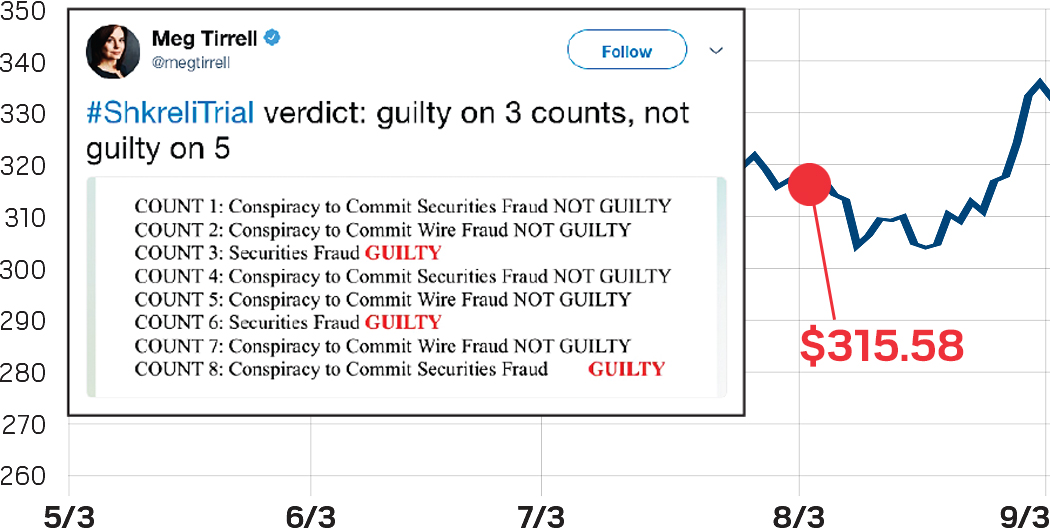
8/4/17
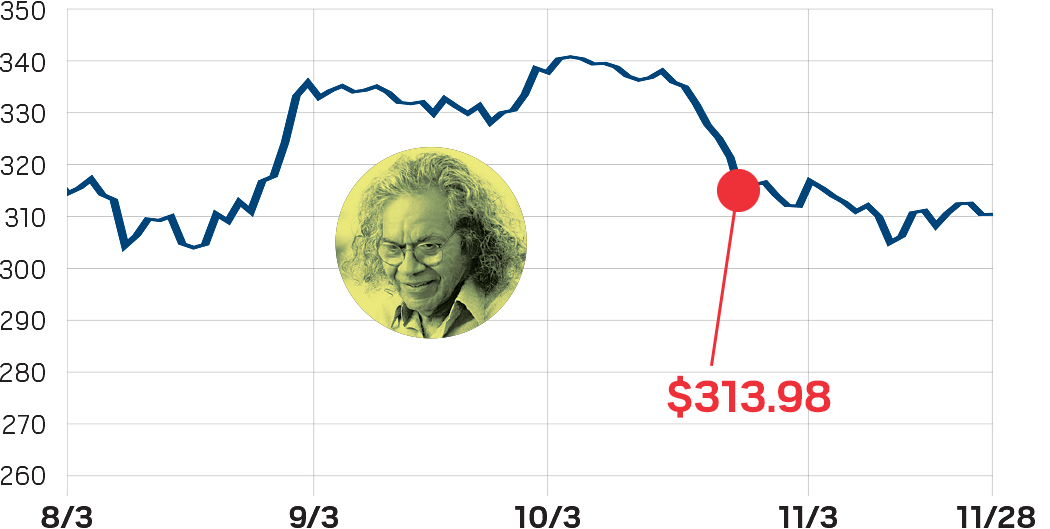
Martin Shkreli is found guilty on three counts in federal fraud case
iShares Nasdaq biotech stock index ($)
8/14/17
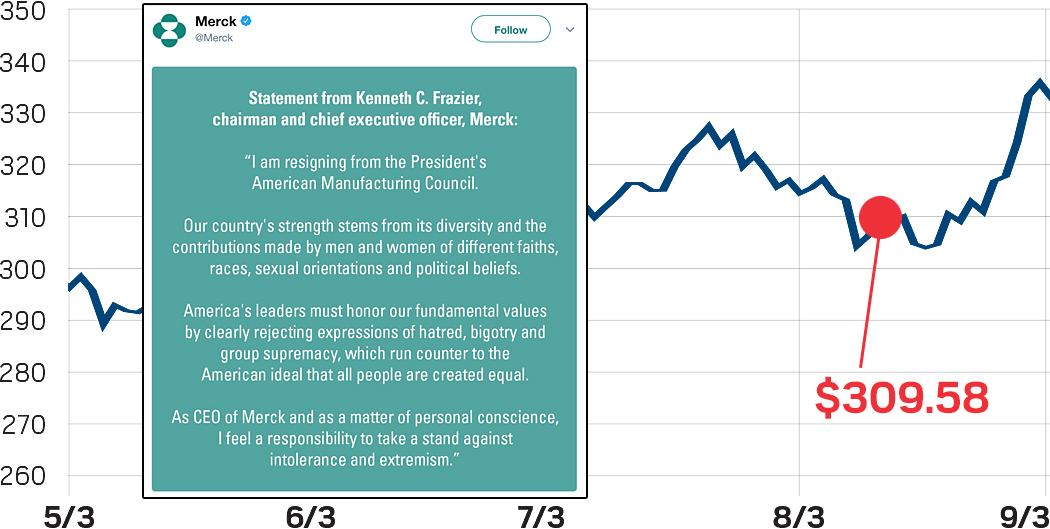
Merck CEO Ken Frazier resigns from Trump’s manufacturing council, prompting others to follow suit
iShares Nasdaq biotech stock index ($)
8/16/17
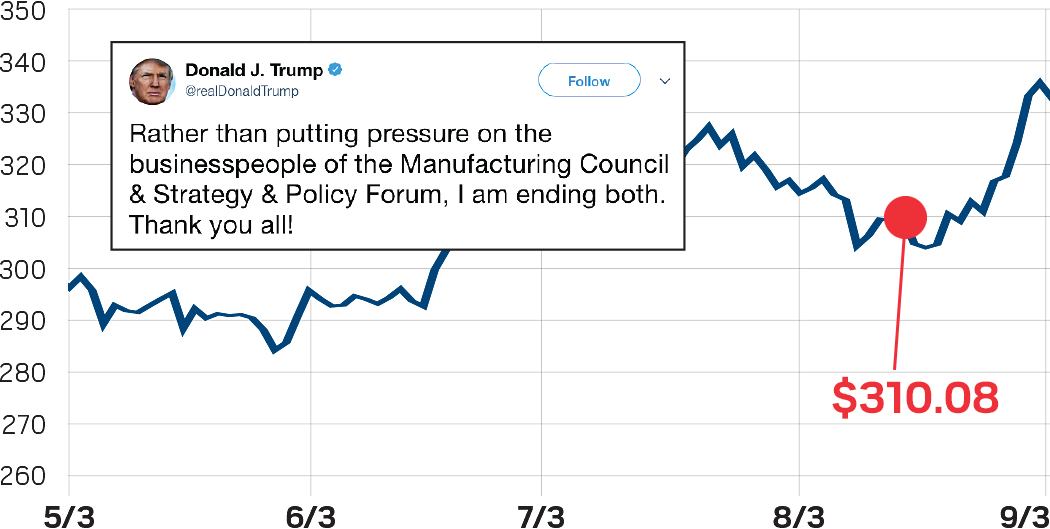
President Trump disbands manufacturing council, which had already lost nearly half its members
iShares Nasdaq biotech stock index ($)
8/28/17
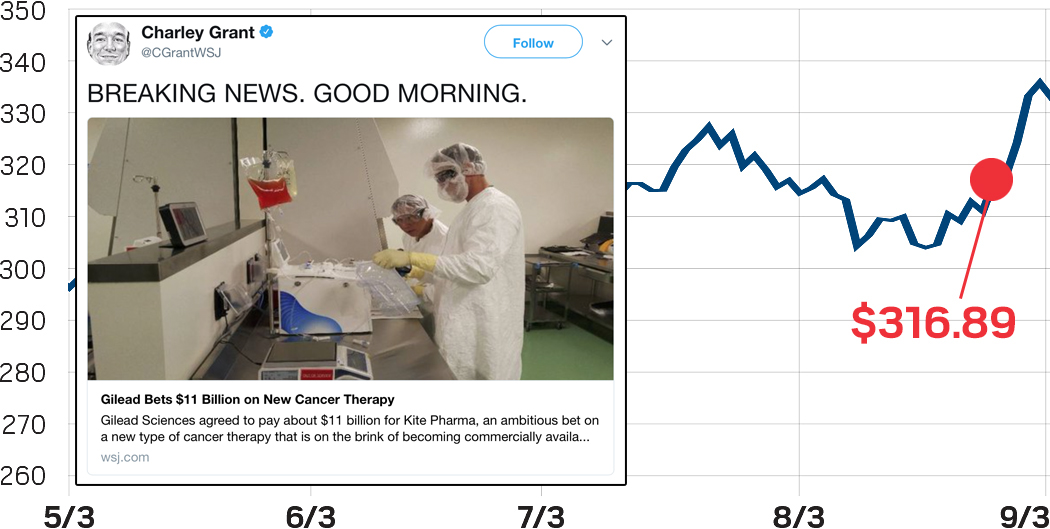
Gilead pays nearly $12 billion for CAR T-cell-focused Kite Pharma
iShares Nasdaq biotech stock index ($)
8/30/17
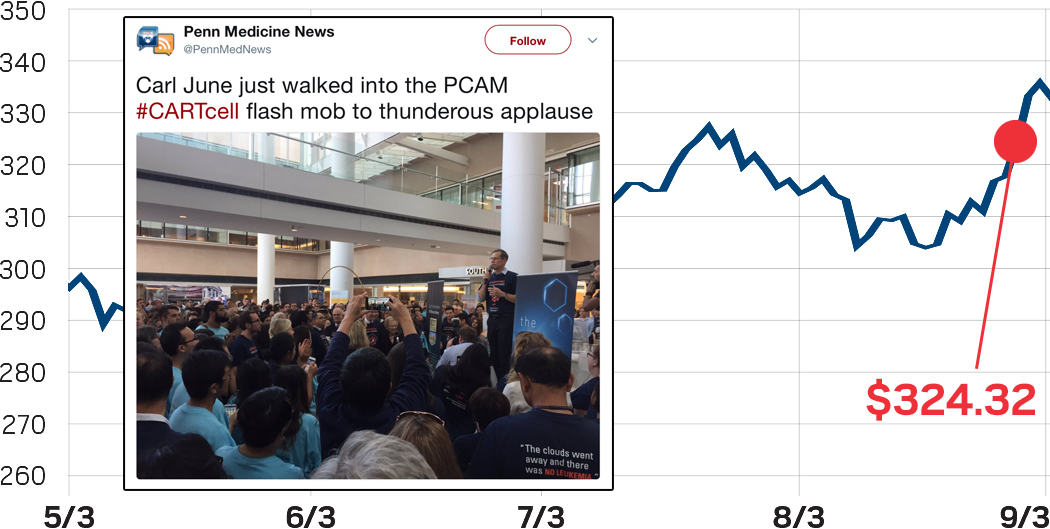
FDA approves first CAR T-cell therapy, Novartis’s Kymriah
iShares Nasdaq biotech stock index ($)
9/8/17
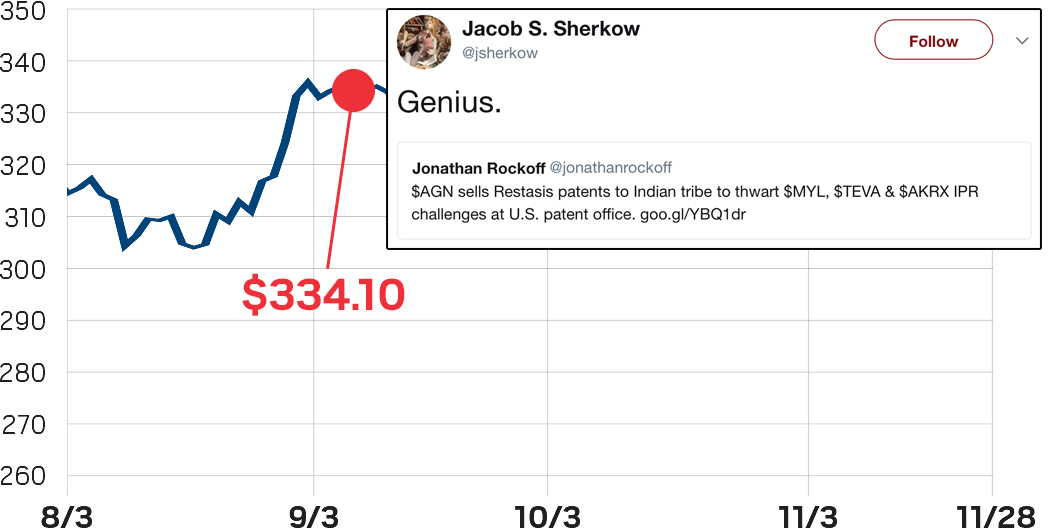
Allergan strikes deal with the Mohawk Tribe with the goal of preventing challenges to patents on its blockbuster eye drug
iShares Nasdaq biotech stock index ($)
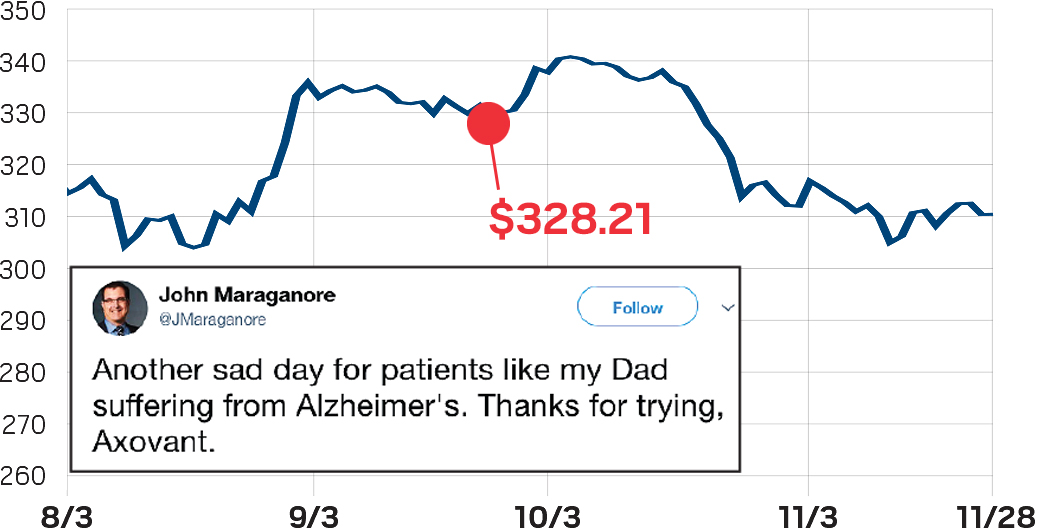
9/26/17
Axovant Sciences’ 5-HT6 agonist intepirdine fails a Phase III study in people with Alzheimer's disease
iShares Nasdaq biotech stock index ($)
9/29/17
Health & Human Services Secretary Tom Price resigns amid criticism over chartered flights
Credit: Shutterstock
iShares Nasdaq biotech stock index ($)
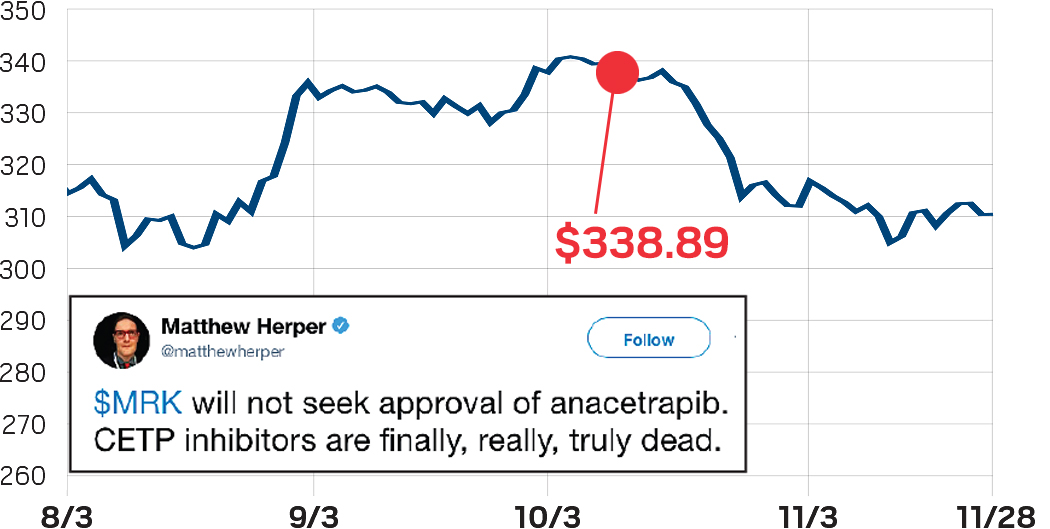
10/11/17
Merck & Co. lets go of anacetrapib, one of a long line of CETP inhibitors for cholesterol to drop out of the drug pipeline
iShares Nasdaq biotech stock index ($)
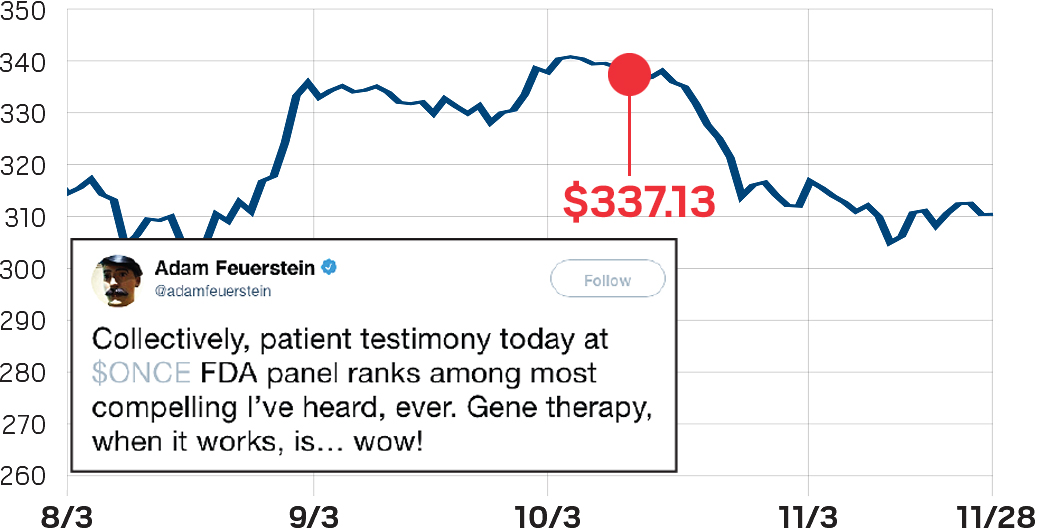
10/12/17
FDA panel votes unanimously to approve Spark Therapeutics’ gene therapy for a rare form of blindness
iShares Nasdaq biotech stock index ($)
10/16/17
Drug stocks drop after Trump says that drug prices “are out of control. The drug prices have gone through the roof.”
iShares Nasdaq biotech stock index ($)
10/18/17
Gilead’s Yescarta is approved, making it the second CAR T-cell therapy on the market
Credit: Gilead
iShares Nasdaq biotech stock index ($)
10/26/17
John Kapoor, founder of fentanyl spray manufacturer Insys Therapeutics, is indicted on racketeering charges
Credit: Newscom
iShares Nasdaq biotech stock index ($)
10/30/17
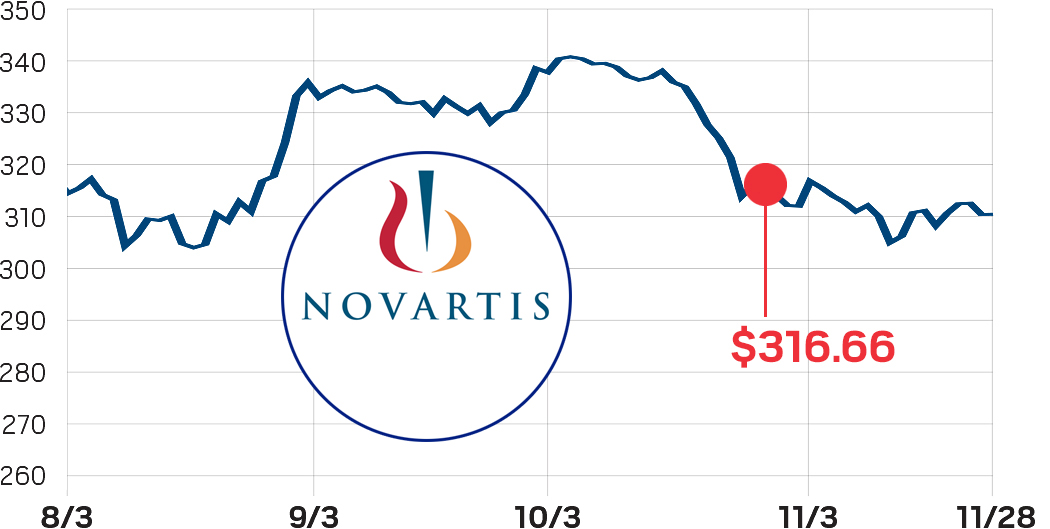
Novartis says it will pay $3.9 billion for radiopharmaceuticals firm Advanced Accelerator Applications
Credit: Novartis
iShares Nasdaq biotech stock index ($)
11/13/17
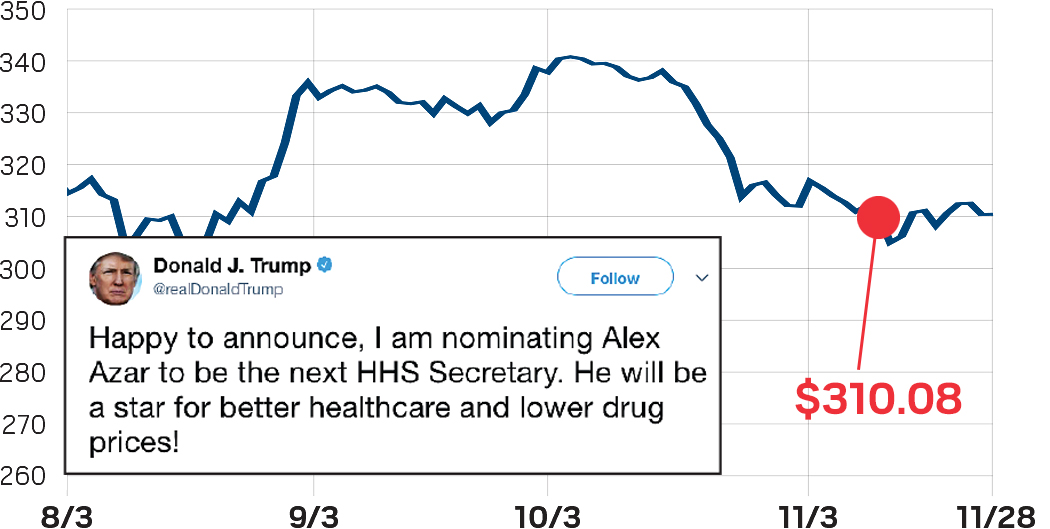
As anticipated, former Lilly executive Alex Azar is nominated as secretary of Health & Human Services
iShares Nasdaq biotech stock index ($)
11/16/17
Alnylam begins the process for asking FDA to approve patisiran, a treatment for familial amyloid polyneuropathy that could become the first RNAi-based drug on the market
Credit: Alnylam
New FDA chief got good marks for his first months
Industry insiders say Gottlieb is good for innovation
When President Donald J. Trump appointed Scott Gottlieb as commissioner of the U.S. Food & Drug Administration, drug industry insiders breathed a collective sigh of relief. Several candidates with little experience in the industry—not to mention unconventional views on the drug approval process—had been floated. Gottlieb, a physician and former deputy commissioner of the agency, was considered an even-handed choice.
Seven months after his confirmation, most continue to believe Gottlieb is the right person for the job. “The general consensus, at least at this point in his tenure, is that he is a breath of fresh air,” says Abbie Celniker, a partner at the venture capital firm Third Rock Ventures. “He is someone who will be driving policy really based on medical need and based on the science behind technologies that are being brought to patients.”
The word many use when describing Gottlieb is balanced. “The conversation is always about benefit and risks, and there have been times in FDA history where risk has been the predominant pole of that axis,” notes Bruce Booth, a partner at Atlas Venture. With Gottlieb, “I think it’s an appropriately balanced view of benefit to risk in transformative medicine.”
Although the price of drugs is not under FDA’s purview, Gottlieb has been more direct than his predecessors in acknowledging the agency’s role in reducing health care costs.
For Gottlieb, that has meant introducing policies to speed the approval of generic drugs and taking steps to thwart artificial monopolies on more-complex generic products, such as the epinephrine auto-injector EpiPen or metered asthma inhalers.
In remarks before the Federal Trade Commission last month, Gottlieb said branded drug firms that exploit loopholes in the system to block generic competition must “end the shenanigans.”
On the other end of the spectrum, Gottlieb has also lamented the unsustainably high cost of developing new drugs. To make the process more efficient, he is calling for modernization of clinical trial design and data collection.
“Scott Gottlieb understands FDA’s role as a catalyst of innovation and is doing what he can to strengthen that role,” says Bernard Munos, a senior fellow at the Milken Institute’s FasterCures research advocacy center. “This is clear from his pronouncements and his moves to speed drug approvals. It’s also clear from his decision to purge FDA’s books of obsolete rules and guidances that slow drug development and increase costs.”
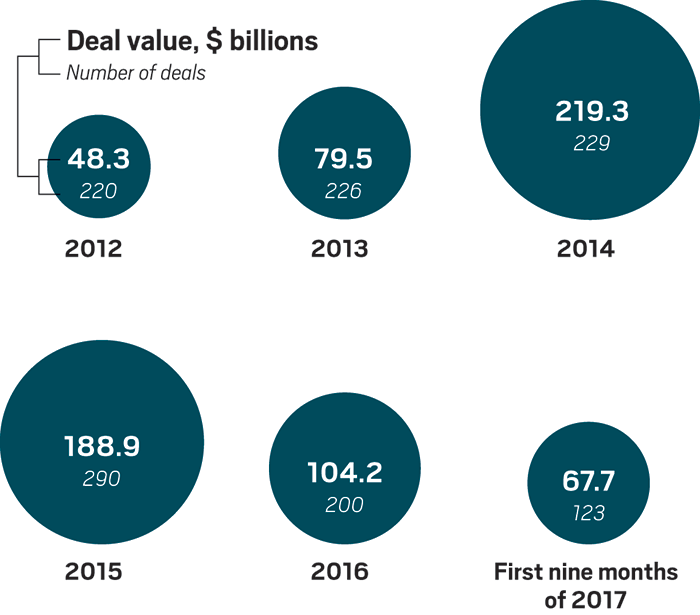
Pharma M&A on pace to hit industry’s ‘new normal’
Industry watchers say activity could pick up in 2018
Merger and acquisition activity in 2017 was relatively healthy, buttressed by two sizable deals: Johnson & Johnson’s $30 billion purchase of Actelion and Gilead Sciences’ nearly $12 billion buy of Kite Pharma.
Although deal-making will not reach the levels hit in 2014 and 2015, it should approach what Ambar Boodhoo, Ernst & Young’s Americas transactions services life sciences leader, calls the “new normal” for the health care sector which, by his firm's definition, includes pharmaceuticals and medical devices. On average, about $200 billion in health care deals get done each year; the tally for the first three quarters of 2017 is $170 billion, Boodhoo says.
That figure could rise in 2018 if the Trump Administration pushes through corporate tax reform, enabling big pharma firms to bring home significant cash that is currently parked overseas.
However, even a flood of capital won’t change the high prices for assets. “I wish I could tell you that things were more realistic and affordable today,” Boodhoo says. “If anything, it has gotten worse.”
Biggest deals in 2017
PURCHASER
TARGET
DEAL VALUEa
MOTIVATION
Johnson & Johnson
Actelion
$30 billion
Pulmonary arterial hypertension portfolio
Gilead Sciences
Kite Pharma
$11.9 billion
Chimeric antigen receptor T-cell therapy (recently approved) and related manufacturing and technology
Takeda Pharmaceutical
Ariad Pharmaceuticals
$5.2 billion
Cancer drugs (two approved pipeline)
Novartis
Advanced Accelerator Applications
$3.9 billion
Radiopharmaceuticals for cancer diagnosis and treatment
Bristol-Myers Squibb
IFM Therapeutics
$2.3 billion
Small molecules targeting innate immune system
Mitsubishi Tanabe Pharma
NeuroDerm
$1.1 billion
Parkinson's disease and other neurological disorder drugs
Ipsen
Merrimack Pharmaceuticals
$1 billion
Cancer treatments
Eli Lilly & Co.
CoLucid Pharmaceuticals
$960 million
Migraine and pain management treatments
Celgene
Delinia
$775 million
T-regulatory modulators for autoimmune diseases
Sanofi
Protein Sciences
$750 million
Non-egg-based vaccines
Merck & Co.
Rigontec
$550 million
Treatments targeting innate immune system
Otsuka Pharmaceutical
Neurovance
$250 million
Attention deficit hyperactivity disorder drugs
Sucampo Pharmaceuticals
Vtesse
$200 million
Rare disease portfolio
a Includes milestones. Source: Company press releases
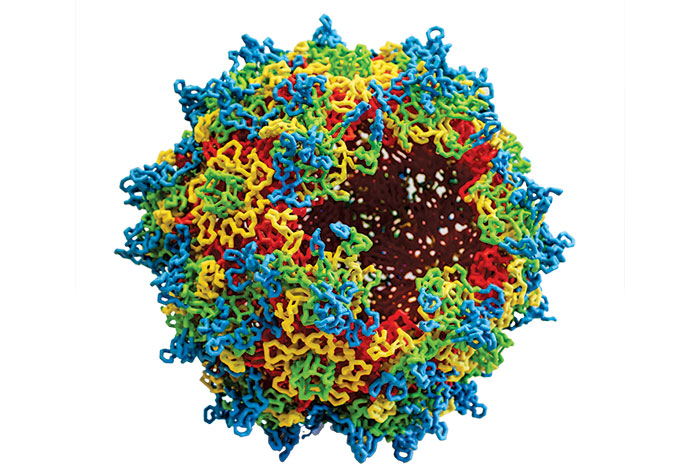
Gene therapy came of age
FDA is expected to approve the first gene therapy, a treatment for a genetic form of blindness, in the U.S. early next year
Credit: Katherine Hinkel/University of Pennsylvania
A model of a hollow adeno-associated virus, which is used to deliver a piece of DNA in gene therapy.
Spinal muscular atrophy type 1 (SMA1) is a diagnosis no parent wants to hear. The rare genetic disease causes muscle wasting and motor neuron death due to a mutation in the SMN1 gene. Infants are too weak to sit up, and most won’t see their second birthday.
The diagnosis for at least 15 babies born with SMA1 is looking different, though, thanks to a clinical trial from Bannockburn, Ill.-based AveXis. Results published last month show that injecting a gene therapy—a healthy copy of the SMN1 gene delivered by an adeno-associated virus (AAV)—has kept the babies, all 20 months or older, alive and kicking (N. Engl. J. Med. 2017, DOI: 10.1056/NEJMoa1706198). Most can now sit up, and some, almost three years old, can even walk and dance.
Geneticists have long been enamored with the idea of treating genetic diseases like SMA by using a virus to deliver a healthy piece of DNA. But getting the technology to work has been a slow process. Despite decades of research, just two gene therapies have been approved for use in Europe, and none have been green-lighted by the U.S. Food & Drug Administration.
The AveXis success story and others like it are now galvanizing the field. Another is Spark Therapeutics’ gene therapy Luxturna, a one-time treatment that allows people with a genetic form of blindness to see better. An FDA advisory board unanimously recommended approval of the drug in October, and the agency is expected to approve it early next year.
Spark and BioMarin Pharmaceutical both have advanced gene-therapy programs to restore genes for the missing blood-clotting proteins in people with hemophilia. Across the industry, over 300 gene-therapy trials are ongoing, and hundreds more are recruiting. “What used to be considered a science experiment is about to become reality,” says AveXis CEO Sean Nolan.
Numerous challenges remain, however, says Guangping Gao, director of the Horae Gene Therapy Center and Viral Vector Core at the University of Massachusetts Medical School. For one, delivering gene therapy throughout some organs, including the lungs, muscles, and brain, is still difficult. And scaling up manufacturing “will be a hard issue to resolve.” Changing current production methods, which are refined but small scale, could diminish the therapy’s potency.
Cost is another concern. Spark has suggested its drug’s one-time price tag could be $1 million. And if a gene therapy doesn’t work the first time, patients are out of luck, since AAV causes an immune response. Some people previously exposed to AAV naturally might also be ineligible for gene therapy.
“I am sure we will have some more setbacks,” says Mark A. Kay, a director of the human gene therapy program at Stanford University School of Medicine. But he is hopeful about the number of treatments that people may soon have access to. “It is an exciting time for gene therapy.”
Another strong year for early-stage biotech investment
Lofty biotech launches covered CRISPR, the microbiome, and more
Life sciences-focused venture capital firms poured significant cash into the drug industry in 2017. Sizable first fundraising rounds for research-driven biotech companies continued, with a handful of platform-based drug discovery companies raking in a ton of cash. Among the notable trends was firms’ attempts to “drug the undruggable”—finding nontraditional ways to access difficult targets. For example, venture-backed companies are using small molecules to block RNA, developing next-generation cellular therapies that can tackle solid tumors, and designing bifunctional small molecules that force unwanted proteins to break down.
SpringWorks Therapeutics
Series A funding: $103 million Focus: Reviving spun-out Pfizer drugs Notable funder: Bain Capital, OrbiMed, Pfizer, LifeArc
KSQ Therapeutics
Series A funding: $76 million Focus: CRISPR-screening platform for oncology and immunology drug discovery Notable funders: Flagship Pioneering, Polaris Partners Notable academic founders: David Sabitini, William Hahn, Jonathan Weissman, Tim Wang
Kymera Therapeutics
Series A funding: $30 million Focus: Targeted protein degradation Notable funder: Atlas Venture
LifeMine Therapeutics
Series A funding: $55 million Focus: Fungal genome mining Notable funder: WuXi Healthcare Ventures Notable academic founder: Greg Verdine
Kaleido Biosciences
Series A & B funding: $65 million Focus: Microbiome Notable funder: Flagship Pioneering
Tango Therapeutics
Series A funding: $55 million Focus: Synthetic lethality Notable funder: Third Rock Ventures
Frequency Therapeutics
Series A funding: $32 million Focus: Hearing loss restoration Notable funder: Cobro Ventures
Vividion Therapeutics
Series A funding: $50 million Focus: Chemical proteomics-based drug discovery Notable funders: Arch Venture, Versant Ventures Notable academic founders: Benjamin Cravatt, Phil Baran, Jin-Quan Yu
Palleon Pharmaceuticals
Series A funding: $48 million Focus: Cancer glycan-based immunoncology drugs Notable funders: SR One, Pfizer Ventures, Vertex Ventures HC, Takeda Ventures, AbbVie Ventures Notable academic founders: Carolyn Bertozzi, Paul Crocker
Arrakis Therapeutics
Series A funding: $38 million Focus: Small molecules targeting RNA Notable funder: Canaan Partners
Disarm Therapeutics
Series A funding: $30 million Focus: SARM1 inhibitors Notable funders: Atlas Venture, Lighthouse Ventures, AbbVie Ventures
Navire Pharma
Series A funding: $30 million Focus: SHP2 inhibitors Notable funder: BridgeBio Pharma Notable academic founder: Benjamin G. Neel Source: Companies
The spotlight was on drug prices, again
Pressure to lower costs ratcheted up as expensive treatments proliferate
Allergan CEO Brent Saunders came under fire for the company’s patent gambit.
When Allergan revealed in September a deal to transfer ownership of patents on its dry-eye drug Restasis to the Saint Regis Mohawk Tribe, the reactions were swift and strong. Designed to block generic competition on a treatment that in 2016 had nearly $1.5 billion in sales, the maneuver was described with adjectives ranging from banal—“unusual” and “unorthodox”—to brutal—“ugly” and “a sham.”
“Company leaders should have killed the idea when they heard it,” says Bernard Munos, a senior fellow at the Milken Institute’s FasterCures research advocacy center. “It is certainly not what the Founding Fathers had in mind when they enshrined intellectual property protection into Article I of the Constitution.”
By exploiting the potential for sovereignty to render the tribe immune from patent challenges, Allergan became the latest face of drug industry greed. It’s a rotating role that often goes to companies jacking up prices on old medicines.
Neither the government nor “the court of public opinion will tolerate bad behavior anymore,” says Thomas Goss, a senior vice president at the consultancy Boston Healthcare Associates.
But it doesn’t take a scandal to be put in the hot seat. New technologies like gene therapy and cancer immunotherapy were lauded this year for their astounding ability to treat, for example, rare genetic diseases or advanced cancers. At the same time, those treatments were called out for their breathtaking prices.
The first chimeric antigen receptor T-cell therapies, a personalized form of cancer immunotherapy, range in price from $373,000 to $475,000. The first gene therapy, expected to be approved in the next two months, could cost as much as $1 million.
With more of these potentially effective—even curative—treatments expected to reach the market in coming years, industry experts anticipate more focus on what they are worth and how to pay for them.
“Greater scrutiny across the board puts pressure on innovators to be sure they’re developing evidence-based value arguments,” Goss says. “Having evidence to support a value proposition is critical in this environment.” Without it, he adds, companies will be challenged to get even novel treatments reimbursed by governments and insurance companies.
Notable drug failures in 2017
Clinical trial failures come with the territory, but late-stage setbacks can have a profound impact on companies and patients
Disappointments and dropouts: Notable failures in pharma’s late-stage drug pipeline.
AMG 899
Company: Amgen Indication: Cholesterol lowering Mechanism of action: CETP inhibitor Modality: Small molecule Phase: II Other: The compound was the centerpiece of Amgen's $300 million acquisition of Dezima Pharma in 2015.
Anacetrapib
Company: Merck & Co. Indication: Cholesterol lowering Mechanism of action: CETP inhibitor Modality: Small molecule Phase: III Other: A 30,000-patient study showed the drug was effective, but Merck concluded it wasn't sufficiently effective to be competitive in the cholesterol-lowering market.
Intepirdine
Company: Axovant Sciences Indication: Alzheimer's disease Mechanism of action: 5-HT6 receptor antagonist Modality: Small molecule Phase: III Other: The compound was licensed from GlaxoSmithKline and had already failed multiple studies.
Mongersen
Company: Celgene Indication: Crohn's disease Mechanism of action: Smad7 protein inhibitor Modality: Oligonucleotide Phase: III Other: Celgene acquired the compound in 2014 from Nogra Pharma for $710 million.
Ozanezumab
Company: GlaxoSmithKline Indication: Amyotrophic lateral sclerosis Mechanism of action: Nogo-A inhibitor Modality: Antibody Phase: II Other: Studies of the drug in multiple sclerosis were previously discontinued.
Serelaxin
Company: Novartis Indication: Heart failure Mechanism of action: Relaxin receptor agonist Modality: Recombinant hormone Phase: III Other: A 6,600-patient study showed the drug did not reduce cardiovascular deaths.
Tralokinumab
Company: AstraZeneca Indication: Asthma Mechanism of action: IL-13 inhibitor Modality: Antibody Phase: III Other: AstraZeneca out-licensed to Leo Pharma rights to develop the antibody to treat skin diseases.
Veliparib
Company: AbbVie Indication: Lung and breast cancers Mechanism of action: PARP inhibitor Modality: Small molecule Phase: III Other: Trials in other types of cancer continue, but veliparib already trails other PARP inhibitors, three of which were FDA approved.
Verubecestat
Company: Merck & Co. Indication: Alzheimer's disease Mechanism of action: BACE inhibitor Modality: Small molecule Phase: II/III Other: Although the drug failed to benefit people with mild to moderate Alzheimer's, Merck is continuing a study of people with a very early form of the disease.
Source: Companies
The opioid crisis got worse
As drug deaths soared, FDA made tough decisions on painkillers
Drug overdose deaths in the U.S. are at an all-time high, and opioids are to blame. According to the latest data from the Centers for Disease Control & Prevention, over 64,000 people died from overdoses in 2016, mostly from opioid painkillers, heroin, and synthetic analogs. That toll cranked up the pressure this year on politicians, law enforcement, and drug companies to respond to the epidemic’s spread.
For its part, the Food & Drug Administration took a harder line on the pain relievers being misused and the companies that manufacture them. Earlier this year, an FDA advisory committee voted 18-8 that the risks outweighed the benefits for an abuse-deterrent version of Endo Pharmaceuticals’ Opana ER painkiller. In a rare move, FDA asked Endo to remove the drug from the market in June.
Undeterred, Endo soon struck a deal with Impax Laboratories to split profits on a generic version of the original Opana ER formulation, which Endo stopped selling in 2010 because it lacked the abuse-deterrent technology. The news prompted FDA Commissioner Scott Gottlieb to announce a study that could lead to restricting the use of oxymorphone, the active ingredient in Opana ER.
The government also went after manufacturers suspected of hiding the risks of opioids. In September, attorneys general in 41 states teamed up to issue subpoenas against Endo and other opioid manufacturers, including Allergan, Janssen Pharmaceuticals, Purdue Pharma, and Teva Pharmaceuticals. Their goal: Determine if the companies deceived doctors and patients about the addictive risks of opioid painkillers.
The crisis has fueled a resurgence of heroin, a cheaper alternative for people who misuse opioids. But synthetic opioids like fentanyl, which is 30-50 times as potent as heroin, now account for the largest number of drug overdose deaths.
In October, President Donald J. Trump declared the U.S.’s opioid problem a national public health emergency, but critics derided Trump’s declaration as mere formality, saying it did little to open up new funds.
Gottlieb has said that solutions to the emergency may include withdrawing more products from the market, reducing the number ofopioid prescriptions, and requiring opioid education for physicians.
The commissioner also wants to expand access to the opioid overdose antidote naloxone and to increase the treatment of addiction with drugs such as methadone or buprenorphine, which are opioids themselves. Two FDA review panels recently recommended approval of weekly and monthly formulations of subcutaneous buprenorphine injections from Indivior and Braeburn Pharmaceuticals to treat opioid use disorder.
“We have a crisis of such massive proportion that the actions we need to take are going to be hard,” Gottlieb told the House Energy & Commerce Committee in October. “Long ago,we ran out of straightforward options.”