Advertisement
Grab your lab coat. Let's get started
Welcome!
Welcome!
Create an account below to get 6 C&EN articles per month, receive newsletters and more - all free.
It seems this is your first time logging in online. Please enter the following information to continue.
As an ACS member you automatically get access to this site. All we need is few more details to create your reading experience.
Not you? Sign in with a different account.
Not you? Sign in with a different account.
ERROR 1
ERROR 1
ERROR 2
ERROR 2
ERROR 2
ERROR 2
ERROR 2
Password and Confirm password must match.
If you have an ACS member number, please enter it here so we can link this account to your membership. (optional)
ERROR 2
ACS values your privacy. By submitting your information, you are gaining access to C&EN and subscribing to our weekly newsletter. We use the information you provide to make your reading experience better, and we will never sell your data to third party members.
Biotechnology
The search for better antivenoms heats up as snakebites get renewed attention
Scientists look for alternative antivenoms that are easy to make and deploy to remote areas
by Dinsa Sachan, special to C&EN
January 28, 2019
| A version of this story appeared in
Volume 97, Issue 4

Credit: EPhotoCorp/Alamy Stock Photo | The Indian cobra (Naja naja) is one of the four most venomous snakes in India.
In brief
More than 100,000 people die every year from venomous snakebites. In 2017, the World Health Organization recognized snakebites as a neglected tropical disease. Some researchers want to tackle the problem by addressing the shortcomings of current antivenoms. These conventional therapies require refrigeration for storage and trained personnel for delivery, both of which rural areas in the developing world often lack. Also, producing the antivenoms involves inoculating horses with snake venoms, which is expensive, is time consuming, and yields proteins that could trigger allergic reactions in people. Several research groups are now developing antivenom alternatives to try to get around these issues.
On a sunny September morning in Nemmara, a small township in Kerala, India, Ally Thomas headed out into the woods. Her plan was to cut grass, feed it to her cattle, and attend a prayer service in the evening—a regular day, by all means. Then a sharp, stinging pain shot through her left foot. A snake had bitten her. The serpent slithered away through the grass before she saw it.
When Thomas reached home, she collapsed with pain. Her family didn’t know what to do. They brought her to a traditional healer, who told her to apply a paste of basil leaves and turmeric on her foot. It didn’t help.
Two days later, she experienced excruciating abdominal pain, her urine turned black, and she spat blood.
Her family took her to a small private hospital nearby. “They told us she was bitten by a very deadly snake and that she might not survive,” recounts Rohan Thomas, Ally’s son.
Doctors at the hospital gave Ally Thomas antivenom, an antidote for snakebites that can save people’s lives if administered quickly enough. In India, doctors give patients a so-called polyvalent antivenom, which targets four of India’s most venomous snake species—Russell’s viper, Indian cobra, saw-scaled viper, and common krait. The hospital hoped giving Thomas this concoction would help her, even though doctors weren’t sure which snake had bitten her. But after the antivenom was administered, Thomas was still in intense pain.
So the next day, her family brought her to the nonprofit Little Flower Hospital and Research Centre, in Angamaly, Kerala. By this time, her limbs were numb and her vision was blurred. Noushad CK, a doctor at the hospital, says Thomas had gone into minor kidney failure, a complication that often arises from the bite of a viper—likely either a Russell’s or pit viper—in this part of the country.
Springing to action quickly, Noushad’s team provided Thomas with intravenous fluids to improve her kidney function, and after two days, her condition improved.

Credit: Dinsa Sachan
Ally Thomas nearly lost her life to the bite of a snake in her hometown of Nemmara in Kerala, India.
“It’s a miracle,” Noushad says. Thomas didn’t receive antivenom until three days after she was bitten. It should be given as soon as possible after a bite. Long delays before receiving antivenom normally result in irreversible organ damage or, worse, death.
As Thomas sat propped up on pillows in the intensive care unit of Little Flower, she expressed how fortunate she felt. “I feel I’ve had a rebirth.”
Although Thomas lived to tell her tale, many in India don’t. Snakebites kill nearly 50,000 people there every year. But snakebites aren’t India’s problem alone. Africa’s snakebite-related mortality rate is estimated at 30,000 per year, with sub-Saharan Africa being most affected. In total, more than 100,000 people die from venomous snakebites around the world each year.
You've got to keep in mind that venom is very complex.
Paulo Lee Ho, biochemist, Instituto Butantan
In June 2017, the World Health Organization took notice, recognizing snakebites as a neglected tropical disease. Since then, the world body has established a working group of researchers, physicians, and public health experts to create a plan for improving access to treatment and improving the quality of antivenoms, especially in the developing world. It also approved a resolution at the World Health Assembly in May 2018 to create a framework for helping countries tackle snakebites.
Many countries struggle with treating snakebites because they lack the infrastructure or logistics planning needed to get antivenoms to people. For example, many clinics in the developing world don’t have adequate facilities for refrigerating antivenom serum. Also, many rural hospitals are often not staffed during the evenings or are remotely located, leaving victims with no choice but to rush to a traditional healer for immediate treatment, just like Thomas and her family did.
Snakebite hot spots
Most venomous snakebites in the world happen in these three regions.
South and Southeast Asia

Estimated venomous snakebites per year:
231,866 – 961,508
Estimated snakebite deaths per year:
14,902 – 52,760

Notable venomous snakes: Russell’s viper (Daboia russelii, shown), Indian cobra (Naja naja), and Malayan krait (Bungarus candidus)
Sub-Saharan Africa

Estimated venomous snakebites per year:
89,009 – 417,343
Estimated snakebite deaths per year:
3,243 – 31,751

Notable venomous snakes: Black mamba (Dendroaspis polylepis, shown), black-necked spitting cobra (Naja nigricollis), and puff adder (Bitis arietans)
Mexico, Central America, and Tropical South America

Estimated venomous snakebites per year:
71,723 – 99,268
Estimated snakebite deaths per year:
293 – 1,760

Notable venomous snakes: Coral snakes (Micrurus, shown), hog-nosed pit vipers (Porthidium), and South American rattlesnake (Crotalus durissus)
Source:PLOS Med.2008, DOI: 10.1371/journal.pmed.0050218.
Another challenge is that some countries lack the expertise to distinguish good antivenoms from bad ones, says Jean-Philippe Chippaux, a French physician who has worked in sub-Saharan Africa. The trouble is, bad ones are often cheaper—and more dangerous. They contain high concentrations of preservatives or protein-degradation products, indicating poor storage conditions, Chippaux says.
Government officials generally pick the more inexpensive antivenom when deciding which one to stock hospitals with, Chippaux adds. “If the criteria is just price, it is not a good thing.” Moreover, not all antivenoms have gone through clinical trials and have therefore not been regulated.
Regulatory concerns aside, some snakebite researchers think antivenoms themselves need an update. The method for making antivenom was standardized in the early 20th century. It involves milking a venomous snake and then immunizing animals, mostly horses, with diluted venom. The horses’ immune systems generate antibodies against the venom molecules over a few months. Technicians then take blood plasma from the horses and extract the antibodies to make the antivenom serum.
It’s a long and expensive process, and some companies cut corners, especially in purification. “In Africa, the purification of antibodies is not sufficiently achieved, and we have antivenom with high risks of side effects,” Chippaux says.
Venoms also contain many components, including peptides, proteins, and enzymes. So antivenoms need to counter combinations of these rather than a single component to be effective. And the antibodies in antivenoms come from horses rather than humans. So injecting them into a person brings with it a risk of an allergic reaction to foreign substances, especially if the purification process hasn’t been carried out properly.
Because of these reasons and more, scientists have started to look for alternatives to current antivenoms, keeping in mind the challenges posed by the poor public health infrastructure in countries such as India.
Skipping the fridge
Some attempts to make alternative antivenoms focus on providing a therapy that is easier to use and easier to store. Current antivenoms are not stable unless refrigerated.
“The major gap in antivenom’s utility is that it can only be administered in the hospital, but the vast majority of deaths from snakebites—upward of 75%—occur before victims can get to the hospital,” says Matthew Lewin, an emergency physician and the director of the Center for Exploration and Travel Health at the California Academy of Sciences.
Lewin’s company, Ophirex, is investigating a therapy that wouldn’t have such storage needs. It is an off-patent compound named varespladib, first developed by the pharmaceutical firm Eli Lilly and Company, for its venom-fighting properties.
The small molecule counters phospholipase A2, an enzyme that is found in the venoms of most snakes around the world. The enzyme degrades the lipids in cell membranes, causing cells to break down and a range of symptoms to appear, including paralysis, bleeding, and muscle destruction. Varespladib binds to the hydrophobic active site of the phospholipase enzyme and destabilizes it so it can’t go to work on lipids. The molecule also appears to fight inflammation in the victim’s body.

In test tubes, varespladib neutralizes the membrane-munching activity of venoms from 28 snake species, including the black mamba and death adder. Intravenous and subcutaneous injections of the molecule led to a 100% survival rate for rats and mice injected with venom from European adders or Eastern coral snakes (Toxins 2016, DOI: 10.3390/toxins8090248). Pigs that have been given coral snake venom also respond to varespladib. All the animals treated with the compound, either orally or intravenously, survived for the period studied, 120 h. But untreated pigs did not (Toxins 2018, DOI: 10.3390/toxins10110479).
The small molecule offers many advantages over conventional antivenoms, Lewin says. It is inexpensive to make and thus would be affordable in resource-poor parts of the world. It would also be shelf stable in tropical climates. Lewin points out that varespladib is thousands of times as potent as a conventional antivenom at inhibiting phospholipase. “Further, it can penetrate tissues that antivenom cannot, such as muscle and neurons.”
But varespladib’s biggest advantage is that anyone can give it to a victim right on the spot after a snakebite, Lewin says. Only trained health-care practitioners can administer traditional antivenom therapy to patients because the agents typically have to be given intravenously, and their side effects need to be monitored.
Still, Lewin emphasizes that the molecule probably would be used in combination with standard antivenoms. “Antivenoms have a longer half-life, circulating longer in the body, and a broader effect on nonphospholipase components of venom,” Lewin explains.
Lewin hopes to begin a Phase I or Pivotal Phase II clinical trial in early 2020, in time for the taipan snakebite season in Papua New Guinea. “We hope to partner with manufacturing firms that have global capabilities so that we can keep costs down and get the drugs to the people that need them most,” Lewin says.
While Lewin is exploring a small-molecule alternative to standard antivenoms, a team led by Kenneth Shea, a chemist at the University of California, Irvine, is investigating a hydrogel consisting of polymer nanoparticles.
The gel works by exploiting a phenomenon that happens when polymer nanoparticles are mixed with a solution containing proteins. The proteins glom on to the particles, creating what is called a corona. Shea and colleagues previously determined that they could get specific proteins to associate with the particles by tuning the composition of their polymers.
So the researchers developed nanoparticles that would form coronas of phospholipase A2, selectively sequestering the enzyme from snake venoms (J. Am. Chem. Soc. 2016, DOI: 10.1021/jacs.6b10950). Shea likes to describe the polymer nanoparticles as plastic antibodies because the particles are plastic and they tie up the enzyme, preventing it from acting on cells.
To find their antivenom nanoparticles, the researchers experimented with different combinations of monomers, such as acrylic acid, N-phenylacrylamide, N-isopropylacrylamide, and N,N′-methylenebis(acrylamide), to produce particles with different polymer compositions. They tested this library of nanoparticles against different types of venoms, and they chose the particles with the highest affinity for phospholipase A2 for further study.
Shea and his team collaborated with José María Gutiérrez of the University of Costa Rica to test the best-performing nanoparticle in mice. They injected venom from an African cobra into the skin of the mice at a dose that would cause skin necrosis. Mice given several doses of the nanoparticle-based gel at the site of venom injection showed no signs of necrosis after 72 h, while untreated mice did (PLOS Neglected Trop. Dis. 2018, DOI: 10.1371/journal.pntd.0006736). According to further studies, the nanoparticles end up in the liver, where they are quickly captured and cleared from the body.
Because the synthetic polymers are stabler than antibodies, this gel could survive in harsh conditions in tropical regions, Shea says. “You don’t have to worry about refrigeration.”
But Shea says this so-called nanodote is not intended to replace traditional antivenom either. “It could be injected directly into the site of the bite by the victim or a companion,” he says. The gel would help keep the victim in stable condition until they get medical help, he adds.
Before moving to clinical trials, Shea and his team want to test the nanodote against other relevant venomous snake species.

Credit: Kenneth Shea
Polymer nanoparticles (left) capture phospholipase A2 (center) and render it inactive.
Biotech lends a hand
While Lewin’s and Shea’s teams are looking for alternatives to antivenoms, some researchers haven’t given up on antivenoms’ main component: antibodies. These scientists are looking to biotechnology to establish less-cumbersome methods of producing venom-deactivating antibodies. The idea is to avoid milking dangerous snakes or injecting venom into horses.
One such approach involves developing human monoclonal antibodies. Monoclonal antibodies are genetically engineered proteins that are synthesized by cloned immune cells and are identical to each other in amino acid sequence. Some cancer therapies use such antibodies to target specific proteins on cancer cells. A human monoclonal antibody is capable of targeting a specific venom toxin. An antidote that is a mixture of monoclonal antibodies could target multiple venom toxins to save the lives of snakebite victims.
Advertisement
If researchers could find monoclonal antibodies that target specific venom ingredients, they could produce the antibodies on a large scale in mammalian cells. “Everything can be produced in big fermentation tanks in the laboratory,” says Cecilie Knudsen, a researcher at the Technical University of Denmark. “This is faster than immunizing animals.” The process takes days, compared with the months that it takes to work with horses.
And because the antibodies are human, they are less likely to cause the allergic reactions seen with antivenoms made using horses. “Moreover, monoclonal antibodies can persist in the human body for a longer time—they don’t get cleared out by the immune system the way foreign antibodies would,” Knudsen says.
What's in a snakebite?
A closer look at five toxins found in snake venoms.
Snake venom metalloproteinases
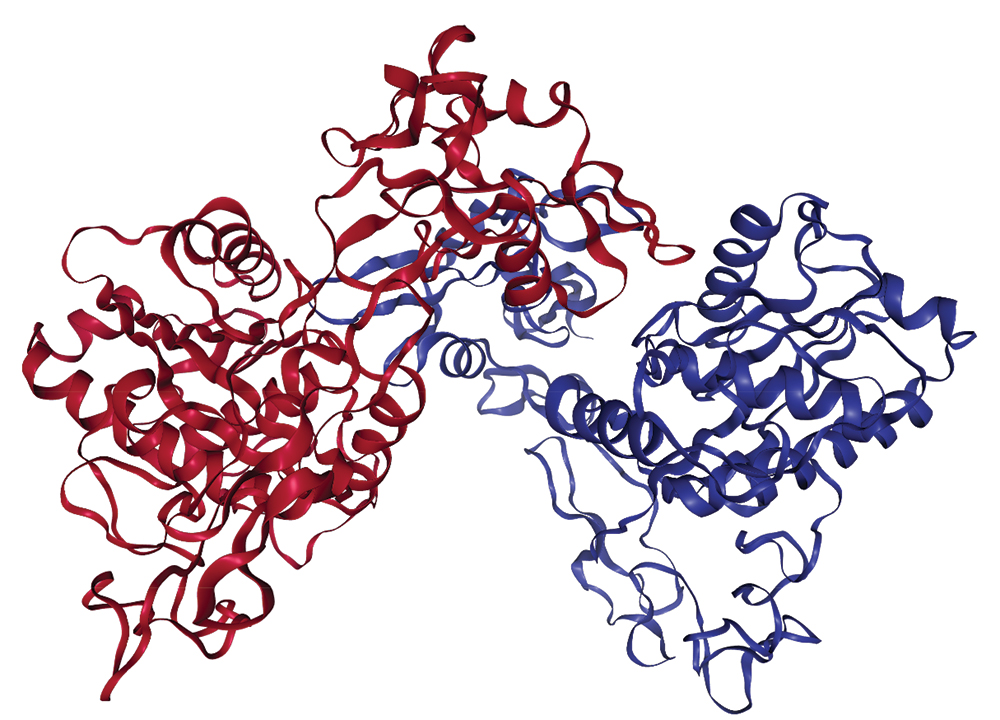
Credit: Protein Data Bank
Snakes with the toxins: Most members of the Viperidae family, including South America’s Bothrops jararaca pit viper
Effects of the toxins: The enzymes produce a wide range of damage. For example, they help cause bleeding by breaking down components of capillaries, and they can disrupt blood clotting.
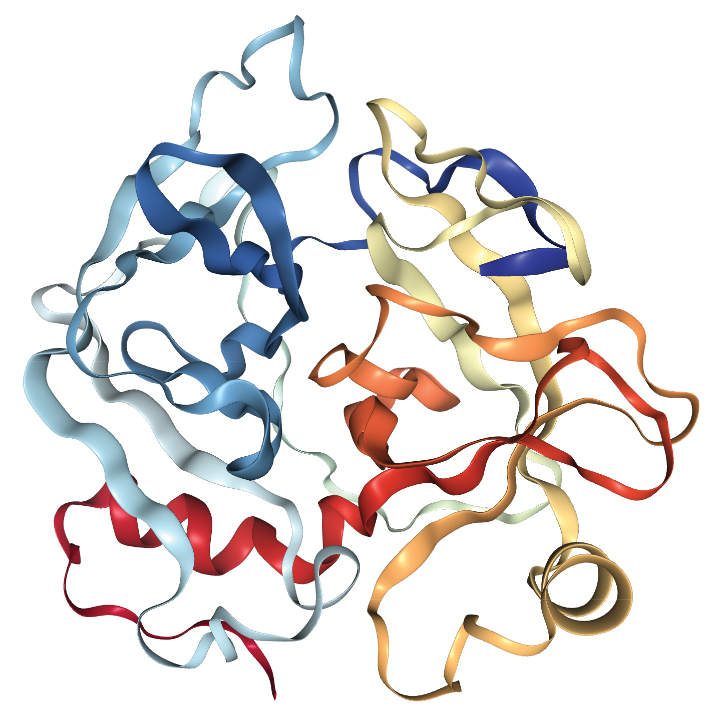
Phospholipase A2

Credit: Protein Data Bank
Snakes with the toxins: Most snakes in the Viperidae and Elapidae families
Effects of the toxins: The enzymes break down the phospholipids in cell membranes, leading to muscle damage and paralysis.
Snake venom serine proteinases
Credit: Protein Data Bank
Snakes with the toxins: Some snakes in both Viperidae and Elapidae families, including the sharp-nosed viper found in southern China
Effects of the toxins: These enzymes disrupt multiple aspects of the blood-clotting process.
Three-finger toxins
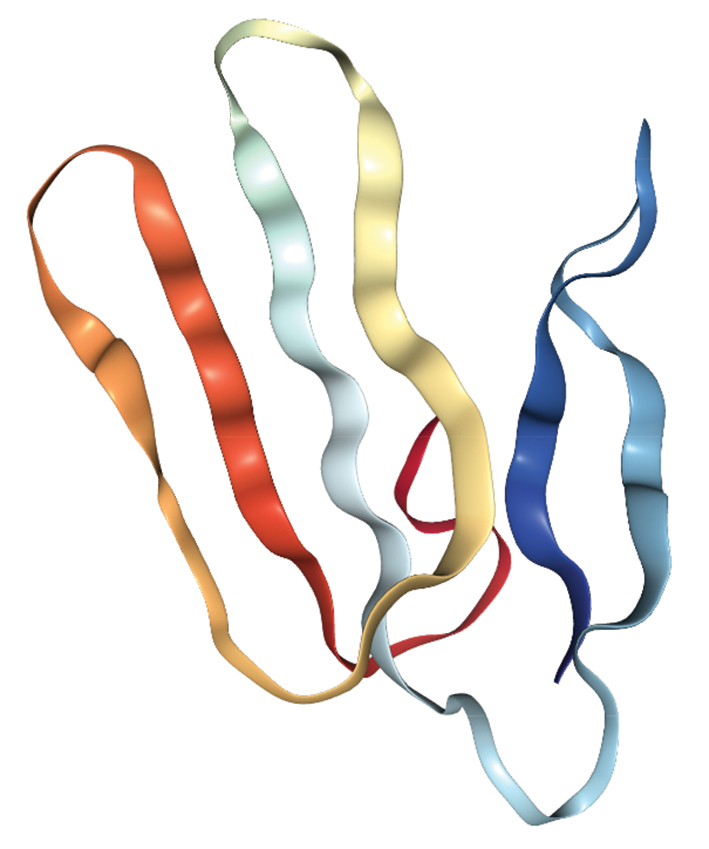
Credit: Protein Data Bank
Snakes with the toxins: Most snakes in the Elapidae family, including the Malayan krait (Bungarus candidus)
Effects of the toxins:These molecules are potent neurotoxins that can cause paralysis.
Dendrotoxins
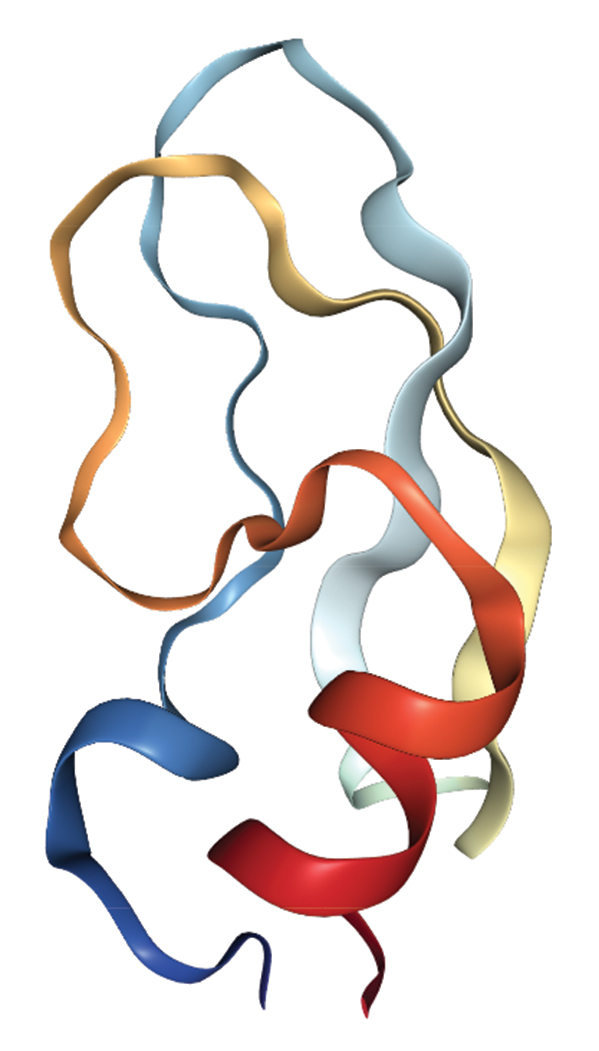
Credit: Protein Data Bank
Snakes with the toxins: Many snakes in the Elapidae family, including the eastern green mamba
Effects of the toxins: These neurotoxins block potassium channels on nerve cells.
Source:Nat. Rev. Dis. Primers 2017, DOI: 10.1038/nrdp.2017.63.
Scientists generally have two approaches to find a human monoclonal antibody that targets a specific venom protein. Hybridoma technology involves injecting the target protein into mice, isolating the genes for the mouse antibody that forms in response to the protein, then tweaking the gene in specific ways to humanize it. The other route is to use phage display, which won the 2018 Nobel Prize in Chemistry, to screen a library of human antibody genes to find the antibody that binds a target protein.
Knudsen and her colleagues from Denmark and Costa Rica used the latter method to find human monoclonal antibodies against the venom of the black mamba, a highly venomous snake from sub-Saharan Africa. They looked for antibodies that could bind to so-called dendrotoxins inside the black mamba’s venom. The team made two prototype antidotes and tested them in mice, finding that treated mice survived injections of the mamba venom (Nat. Comm. 2018, DOI: 10.1038/s41467-018-06086-4).
Black mamba venom contains another group of deadly components called α-neurotoxins. Knudsen’s team next wants to develop antibodies against those molecules. The researchers’ goal is to find antibodies for all the key mamba toxins and then mix them together into one antidote.
Meanwhile, Paulo Lee Ho, a biochemist at Instituto Butantan, in São Paulo, and his team are also harnessing biotechnology techniques to derive an antivenom against a particularly tricky snake. Their target is the venom of the coral snake Micrurus corallinus, one of the deadliest serpents in Brazil.
“The problem with making antivenom against coral snake is obtaining venom to immunize the horse. It doesn’t have enough venom in the venom gland,” Ho says.
Instead of milking these snakes for their paltry supply of venom, the team wanted to find a way to make the proteins themselves. They examined the amino acid sequences of the venom’s five most important toxins and then mapped their epitopes—the parts of the toxins to which an antibody would actually bind. They then constructed genes that encoded just those epitopes.
The researchers injected pieces of DNA containing these genes into mice so that the animals’ cellular machinery would synthesize and churn out proteins containing the epitopes. The rodents’ immune systems then started to produce antibodies against these epitopes. Basically, the scientists used the pieces of DNA to immunize the mice against the venom—like injecting horses with the actual snake toxins.
The team found that immunizing the mice first with these DNA pieces and then with a booster shot of proteins containing just the epitopes was fairly successful. The animals’ survival rate when injected with the snake venom was 60%. All the untreated mice died.
Ho wants to improve the survival rate. He thinks that the researchers haven’t yet isolated epitopes for all the significant toxins in the coral snake’s venom. “You’ve got to keep in mind that venom is very complex.”
Ho thinks this epitope immunization method could work well for snakes that have limited amounts of venom or highly venomous serpents that are difficult to handle. To produce antivenoms for people rather than mice, the team would have to apply its technique to horses and harvest the antibodies produced after immunizing them.
A long wait ahead
Some antivenom researchers are excited about these alternatives but think it’s still early days in their development. In particular, Chippaux, the French physician, thinks it will take a while for monoclonal antibodies to make it to the clinic for testing against snakebites. The venom of a single species of snake, he says, contains an eclectic cocktail of toxins, and making antibodies against every one of them would be a marathon task.
Julien Potet, a policy adviser for the nonprofit group Doctors Without Borders, says in the near term, these alternatives could work in conjunction with current antivenom therapies. For example, he says, monoclonal antibodies “could be added to the conventional animal antibody preparations in order to fortify them against selected snake venoms that are hard to neutralize with existing products.”
In general, these novel antidotes will have to prove a lot before they’d be adopted in the field, experts say. First, Potet says, other researchers will need to confirm in the lab that the antidotes neutralize their targeted venoms. After that, scientists will need to investigate any possible toxicities of the novel agents. And then large-scale clinical trials will be needed, and those are expensive.
“You need detailed studies that involve thousands of people for these novel antidotes because venom works differently on different people’s bodies, based on individual height, body weight, and amount of venom injected,” says Priyanka Kadam, founder of the India-based nonprofit group Snakebite Healing and Education Society and a member of the WHO panel on venomous snakebites.
Unfortunately, most of the antivenoms that are supplied to sub-Saharan Africa and India aren’t clinically tested. “Like for other neglected tropical diseases, there is very limited funding for the development of antivenoms,” Potet says. “For many producers, the money is just not there to finance the clinical trials. Only a couple of the dozen existing antivenoms intended for use in sub-Saharan Africa have been evaluated in robust randomized clinical trials.” And that doesn’t stop countries with lackadaisical regulatory bodies from registering antivenoms anyway. “It’s a shame,” Potet says.
Meanwhile, Chippaux, who has treated snakebites in sub-Saharan Africa for decades, believes there is actually no need for novel antidotes. Just improving the quality and quantity of conventional antivenoms could significantly help Africans. “There is a need for a greater quantity of good-quality antivenom. While fewer than 100,000 doses are sold annually in sub-Saharan Africa, actual needs are estimated to be higher than 1 million doses,” he says.
Potet also urges antivenom manufacturers to keep improving the current inventory. “This is not rocket science, and the investments that need to be made are probably not very high, but they need to happen,” Potet says.
He points to incremental improvements at all stages of antivenom production, including how the venom immunization mixture is prepared and how the final product gets purified. “Not many producers have focused on these incremental improvements,” he says.
In 2016, the WHO commissioned an assessment of the antivenoms sold in Africa and the facilities, many of which are in India, where they are produced. Manufacturers were asked to submit information about their products to the organization. WHO officers also inspected the facilities to check if they followed best practices of production—for example, they determined whether the horses were kept in healthy conditions. The WHO hasn’t yet disclosed its findings but plans to release a list of trusted suppliers after this assessment. “This will clarify which antivenoms are the most capable of neutralizing the venoms of the different African snake species,” Potet says.
Moreover, Doctors Without Borders is gearing up to host and implement clinical trials of existing antivenoms in sub-Saharan Africa because it wants to find the most effective antivenoms for African snake species. The organization will start after the WHO completes its assessment of African antivenoms. “Once this assessment is finalized, we will be able to select the antivenoms that we’d like to test in our clinical trial,” Potet says.
Like for other neglected tropical diseases, there is very limited funding for the development of antivenoms.
Julien Potet, policy adviser, Doctors Without Borders
No matter which of these efforts—improving current antivenom production, developing antivenom alternatives, or creating human-antibody-based antivenoms—is most successful, it’s clear that changes are needed. “Ninety-five percent of people affected by snakebites come from impoverished backgrounds, and they aren’t aware of their fundamental rights, including the right to basic health care,” Kadam says. “These are voiceless victims, and not a priority for policy makers.” She says the developing world badly needs a novel antidote that could reduce treatment costs. “It would be a game changer.”
Dinsa Sachan is a freelancer writer based in New Delhi.
CORRECTION: This story was updated on Feb. 6, 2019, to correct an editorial error that led to an inaccurate representation of a statement by Matthew Lewin. He said that more than 75% of deaths from snakebites occur before victims get to a hospital.
Chemical & Engineering News
ISSN 0009-2347
Copyright © 2024 American Chemical Society
You might also like...



The power is now in your (nitrile gloved) hands
Sign up for a free account to get more articles. Or choose the ACS option that’s right for you.
Already have an ACS ID? Log in
Join the conversation
Contact the reporter
Submit a Letter to the Editor for publication
Engage with us on Twitter